Meningiomasare the most frequently reported primary intracranial neoplasms in the US. Most of these lesions are benign (i.e., WHO Grade I) with a low tendency for invasion and recurrence and a natural history of slow growth. Within the intracranial space, there is a narrow capacity for mass expansion. The primary approach for large meningiomas has been resection. Despite a dramatic decline in surgical morbidity for meningiomas reported over the last 2 decades, gross-total resection of meningiomas in critical locations, especially the skull base, has remained a challenge, and patients often require multiple surgeries leading to increased morbidity and mortality.6,10,36In recent years, primary or adjuvant treatment with stereotactic radiosurgery (SRS) has gained favor. SRS has demonstrated its safety and efficacy in the control of benign tumors, particularly for small to moderately sized meningiomas. Tumor control rates for WHO Grade I skull base meningiomas after SRS average approximately 91% and 88% at 5 and 10 years, respectively.13,19,22,27,33–35,38,39,48,51
Most meningioma radiosurgical series have excluded large volume tumors. Traditionally, a tumor diameter of 30–35 mm was the recommended cutoff for radiosurgery.30–32在先前的研究中,大脑膜瘤胎面ted with varying degrees of success, but radiosurgery outcomes appear to worsen for patients harboring meningiomas greater than 8 cm3in volume.8,15,16,20,42An 8-cm3volume corresponds to a lesion with an approximate diameter of 2.5 cm. Radiosurgery to lesions in excess of 8-cm3volume has been linked to worsening outcome with arteriovenous malformations, acoustic neuromas, and brain metastases as well.12,18,26In the present study, we retrospectively reviewed data of patients harboring large WHO Grade I skull base meningiomas (volume > 8 cm3) who were treated with single-session Gamma Knife radiosurgery (GKRS) to identify prognostic factors associated with successful and adverse radiological and clinical outcomes.
开云体育世界杯赔率
Patient Population
This is a retrospective analysis of a prospectively maintained database approved by the University of Virginia institutional review board. The database was assessed from 1989 to 2013 for patients with skull base meningiomas treated with single-session GKRS at the University of Virginia (n = 469). The diagnosis was confirmed either by tissue pathology or characteristic findings for meningiomas on neuroimaging studies. Tumors typically exhibited radiological features of a meningioma including dural base, extraaxial location, uniform contrast enhancement, and intratumoral calcification. Exclusion criteria included patients with multiple meningiomas, history of prior cancer, follow-up less than 6 months unless there was a complication, and a confirmed tumor histological grade greater than WHO Grade I. All patients with tumor progression and all those with complications following GKRS were included, regardless of follow-up duration. Consequently, 75 patients had large tumors (> 8 cm3) as assessed with tumor volumetry using radiosurgical planning software at the time of GKRS and were included for analysis.
Patients were considered for GKRS if they were not disabled by their tumor, i.e., Karnofsky Performance Scale score < 70. For those who underwent upfront treatment with GKRS, patients were not candidates for primary resection based upon their advanced age, the projected operative risks based on medical comorbidities, and/or refusal of microsurgical resection. Adjuvant radiosurgery was performed in patients with recurrence of lesions following microsurgical excision or as part of multimodality treatment whereby the risks of surgical gross-total resection outweighed the benefits of multimodality therapy.
Patient and Tumor Attributes
Of the 75 patients with large skull base meningiomas, 51 were female (68%) and 24 were male (32%), with a median age of 55 years (range 19–85 years). Forty-five patients (60%) had a history of surgery and histologically confirmed WHO Grade I meningiomas, while the remaining 30 patients treated with upfront radiosurgery had neuroimaging characteristics and a clinical history consistent with a benign meningioma (40%). Alteration in function of cranial nerves (CNs) III, IV, V, or VI was the most common neurological deficit on presentation. The mean volume of tumors prior to radiosurgery was 14.1 ± 6.7 cm3(median 12.4 cm3, range 8.1–54.8 cm3). The parasellar region (n = 42, 56%) and cerebellopontine angle (CPA) (n = 10, 13%) were the most common tumor locations. Preoperative patient characteristics, presentations, and tumor characteristics are detailed inTable 1.
Baseline characteristics of 75 patients with large skull base meningiomas treated with GKRS
| Characteristic | Value (%) |
|---|---|
| Females | 51 (68) |
| Age (yrs) | |
| Median ± SD | 55 ± 13 |
| Range | 19–85 |
| Previous resection | 45 (60) |
| Previous radiotherapy | 4 (5) |
| Previous GKRS | 3 (4) |
| Initial presentation* | |
| Headache | 18 (28) |
| Subjective dizziness | 14 (22) |
| Seizure | 3 (5) |
| CN | |
| III/IV/VI | 29 (45) |
| V | 33 (52) |
| VII | 9 (14) |
| VIII | 11 (17) |
| IX/X | 1 (2) |
| XI | 0 (0) |
| XII | 1 (2) |
| Hypopituitarism | 2 (3) |
| Body weakness | 4 (6) |
| Dysgraphia | 2 (3) |
| Cognition | 1 (2) |
| Location | |
| Parasellar | 42 (56) |
| Petroclival | 9 (12) |
| Clival | 6 (8) |
| Tentorial | 3 (4) |
| CPA | 10 (13) |
| Petrous | 2 (3) |
| Sphenoidal | 2 (3) |
| Jugular foramen | 1 (1) |
| Tumor volume (cm3) | |
| Mean ± SD | 14.1 ± 6.7 |
| Range | 8.1–54.8 |
| Tumor diameter (cm) | |
| Mean maximum | 3.8 ± 0.8 |
| Range | 2.5–6 |
| Edema on pre-GKRS imaging | 4 (5) |
Clinical presentation data available for 64 patients.
Radiosurgical Technique
Our radiosurgical technique has been previously described.49In brief, patients underwent placement of a stereotactic Leksell model G stereotactic frame (Elekta Instruments Inc.) in the operating room. During frame placement, they received monitored anesthesia administered by an anesthesiologist. Stereotactic MRI was then obtained for the treatment planning. Pre- and post-contrast thin-slice (1-mm) volume acquisition axial and coronal MRI sequences were obtained. When an MRI was not able to be obtained due to medical contraindications (e.g., a cardiac pacemaker), a thin-slice stereotactic CT scan was obtained with and without contrast administration. Radiosurgical dose plans were formulated under the direction of a neurosurgeon in conjunction with a medical physicist and radiation oncologist. In general, the maximum dose to the optic apparatus was kept to 8 Gy or less. The Leksell Gamma Unit Model U was used until July 2001 when the C model (Elekta Instruments, Inc.) was instituted. The Gamma Knife Perfexion unit has been used to treat patients since 2007. The Kula software was used for dose planning from 1990 to June 1994, and then subsequently Elekta's Gamma Plan software was used. All patients in this series were treated with single-session radiosurgery. Initial tumor volume was assessed by contouring and then using Gamma Plan software.
Gamma Knife Radiosurgery Parameters
The mean dose to the tumor margin was 13.5 ± 3.5 Gy (range 4.8–30 Gy) with a mean maximal dose of 31 ± 5 Gy (range 23–40 Gy). Only 1 patient received a marginal dose of less than 9 Gy, and the 5th to 95th percentiles for marginal dose ranged from 9 to 20 Gy. The majority of tumors were treated with multiple isocenters (mean 13 ± 10 isocenters, range 1–43 isocenters) to the mean prescription isodose line of 42% ± 9% (range 30%–55%). Radiosurgery parameters are detailed inTable 2.
GKRS treatment parameters
| Characteristic | Mean ± SD (range) |
|---|---|
| Margin dose (Gy) | 13.5 ± 3.5 (4.8–30) |
| Maximum dose (Gy) | 31 ± 5 (23–40) |
| Isodose line (%) | 42 ± 9 (30–55) |
| No. of isocenters | 13 ± 10 (1–43) |
Clinical and Radiological Follow-Up
Patients were routinely followed clinically and radiologically every 6 months for the first year, annually until 5 years after radiosurgery, and then every 2 years thereafter. At each follow-up visit, a neurological examination was performed to evaluate for new neurological deficits, and neuroimaging studies were reviewed to assess tumor response by both a neurosurgeon and neuroradiologist. All follow-up evaluation was performed at the University of Virginia, unless the patient was unable to travel to our institution. In such cases, the referring physician performed the follow-up and provided documentation of the patient's neurological status, as well as follow-up imaging.
All neuroimaging studies were reviewed by a neurosurgeon and a neuroradiologist at the University of Virginia. Lesions were categorized into the following locations defined by the presumed origin of maximal volume: sellar or parasellar, CPA, petrous, clival, petroclival, jugular foramen, and sphenoid.2,3,5,50,54,55Petroclival meningiomas were defined as tumors whose maximal volume was centered over the region between the petrous apex and the upper two-thirds of the clivus.3,50All parasellar lesions were in close proximity to the sella with cavernous sinus invasion.54
Imaging outcome was determined by the last available radiological examination by a neurosurgeon and a neuroradiologist.47A decrease or increase in tumor size was defined as a 15% or greater change in tumor volume as compared with the volume at the time of GKRS.47Tumors with less than a 15% change from their initial volume were considered radiologically stable. Any patient with tumor progression of greater than 15% was considered a treatment failure even if this stabilized with further GKRS or surgery.47To make the determination of tumor volume, the tumor was outlined on radiological images and serial volumetric calculations were performed using Image J in all patient imaging studies (NIH).47The presence of perilesional edema was defined as FLAIR or T2-weighted changes around the tumor. These changes were evaluated by a neuroradiologist (M.S.) who assessed the radiosurgical planning MR images and the follow-up MR images for the presence of baseline edema and an exacerbation of the same after radiosurgery.
Statistical Analysis
Data are presented as median or mean and range for continuous variables, and as frequency and percentage for categorical variables. Calculations of normality were performed by ladder of powers and assessed graphically. Statistical analyses of categorical variables were conducted using chi-square, Fisher's exact, and Mantel-Haenszel tests for linear association as appropriate. Statistics of means were performed using an unpaired Student t-test, both with and without equal variance (Levene's test) as necessary and Wilcoxon rank-sum tests when variables were not normally distributed. The following dependent variables were assessed in univariate and multivariate analysis: tumor-free progression, worsening or new decline in neurological function, and favorable outcome (no tumor progression or worsening or new decline in neurological function). Kaplan-Meier risk of tumor progression was calculated. Factors predictive of tumor progression (p < 0.20)4进入多变量Cox回归肛交吗ysis to assess hazard ratios (HRs). Clinical covariates predicting new or worsening decline in neurological function with a univariate p value < 0.20 were included in multivariable logistic regression analysis. Additionally, clinical covariates predicting unfavorable outcome with a univariate p value < 0.20 were included in multivariable logistic regression analysis. Clinically significant variables and interaction expansion covariates were further assessed in both Cox and logistic multivariable analysis as deemed relevant. Youden indices were calculated to determine cutoffs for the dichotomized continuous variable tumor volume that yielded the optimal discrimination of tumor progression and overall outcome. Those p values ≤ 0.05 were considered statistically significant.
Results
Clinical Outcomes
Detailed clinical follow-up data were available for 64 patients. Neurological function was unchanged in 37 patients (58%), improved in 16 patients (25%), and declined in 11 patients (17%). Specific alterations in neurological function are displayed inTable 3. The most common CNs to have new or worsening function following GKRS were II, III, and V, which each occurred in 4 patients (6%). Additionally, the most likely CNs to demonstrate improvement following GKRS were III, V, and VII occurring in 3 (5%), 4 (6%), and 3 (5%) of patients, respectively. In the current series, there was no evidence of vascular injury or brainstem ischemia as a result of SRS.
Neurological outcomes for 64 patients with large skull base meningiomas treated with GKRS
| Variable | Deficit Before GKRS | Stable Deficit | Improved Deficit | Worsened or New Deficit |
|---|---|---|---|---|
| Total patients (%) | 59 (92)* | 37 (58)† | 16 (25) | 11 (17) |
| Total no. of deficits per patient (%) | ||||
| Dizziness | 14 (22) | 12 (19) | 2 (3) | 0 |
| Body weakness | 4 (6) | 3 (5) | 1 (2) | 0 |
| Seizure | 3 (5) | 3 (5) | 0 | 1 (2) |
| Hypopituitarism | 2 (3) | 2 (3) | 0 | 0 |
| Dysgraphia | 2 (3) | 2 (3) | 0 | 0 |
| Cognition | 1 (2) | 0 | 1 (2) | 1 (2) |
| CN deficit* | 52 (81) | 33 (52) | 12 (19) | 9 (14) |
| CN I | 2 (3) | 2 (3) | 0 | 0 |
| CN II | 19 (30) | 15 (23) | 1 (2) | 4 (6) |
| CN III | 24 (38) | 18 (28) | 3 (5) | 4 (6) |
| CN IV | 3 (5) | 3 (5) | 0 | 1 (2) |
| CN V | 33 (52) | 26 (41) | 4 (6) | 4 (6) |
| CN VI | 16 (25) | 16 (25) | 0 | 1 (2) |
| CN VII | 9 (14) | 6 (9) | 3 (5) | 0 |
| CN VIII | 11 (17) | 10 (16) | 1 (2) | 0 |
| CN IX | 0 | 0 | 0 | 0 |
| CN X | 1 (2) | 0 | 1 (2) | 0 |
| CN XI | 0 | 0 | 0 | 0 |
| CN XII | 1 (2) | 1 (2) | 0 | 0 |
Some patients had multiple deficits
Includes patients who did not present with a deficit.
Predictors of new or worsening decline in neurological function in univariate analysis are demonstrated inTable 4. In multivariate analysis, the factors predictive of new or worsening decline in neurological function were history of surgery (OR = 3.00, 95% CI 1.13–7.95; p = 0.027), presentation with any CN deficit from III to VI (OR = 3.94, 95% CI 1.49–10.24; p = 0.007), and decreasing maximal dose (OR = 0.76, 95% CI 0.63–0.93; p = 0.007). Tumor progression was present in 7 (64%) of 11 patients with new or worsening decline in neurological function.
Predictors of new or worsening neurological deficits
| Predictive Factor | OR | 95% CI | p Value |
|---|---|---|---|
| Univariate analysis* | |||
| Location | |||
| All other locations | 1.00 | ||
| Parasellar/petroclival | 7.10 | 0.85–59.54 | 0.071 |
| History of radiotherapy | 6.25 | 1.07–36.54 | 0.042 |
| History of surgery | 2.40 | 1.08–5.34 | 0.032 |
| Any CN deficit from III to VI | 2.98 | 1.43–6.23 | 0.004 |
| Seizure | 11.56 | 0.95–141.13 | 0.055 |
| Increasing volume | 1.06 | 0.98–1.15 | 0.171 |
| Decreasing peripheral dose | 0.82 | 0.64 - -1.05 | 0.118 |
| Decreasing maximal dose | 0.83 | 0.71–0.96 | 0.012 |
| Multivariate analysis | |||
| History of surgery | 3.00 | 1.13–7.95 | 0.027 |
| Any CN deficit from III to VI | 3.94 | 1.49–10.24 | 0.007 |
| Decreasing maximal dose | 0.76 | 0.63–0.93 | 0.007 |
Factors predictive of new/worsening symptoms (p < 0.20).
Radiological Outcome
The mean follow-up duration was 6.5 years (range 0.5–21 years). During this time, 37 patients (49%) displayed no change in tumor volume, 26 (35%) had decreased volume, and 12 (16%) displayed increased volume. Kaplan-Meier analysis demonstrated radiological progression-free survival at 3, 5, and 10 years to be 90.3%, 88.6%, and 77.2%, respectively (Fig. 1).

Graph of tumor-free progression after GKRS.
Four patients had a history of edema prior to SRS (5.3%). Following radiosurgery, 4 patients had new or worsening edema within 18 months of treatment: 1 patient had progression of preexisting edema and 3 patients developed edema following SRS. The edema improved in 1 patient following a short course of steroids but persisted in the other 3 patients. Three patients with preexisting edema experienced improvement in the edema following radiosurgery. There were no cases of malignant transformation of an existing meningioma or radiation-induced secondary tumor development.
Factors predictive of tumor progression in univariate analysis are displayed inTable 5. Prior resection was not predictive of tumor control (Fig. 2). Regarding tumor control, Youden indices demonstrated that the optimal breakpoint for tumor volume occurred at 14 cm3(Fig. 3). In the Cox multivariable analysis, the covariates associated with tumor progression included presentation with any CN deficit from III to VI (HR = 3.78, 95% CI 1.91–7.45; p < 0.001), history of prior radiation therapy (HR = 12.06, 95% CI 2.04–71.27; p = 0.006), and tumor volume greater than 14 cm3(HR = 6.86, 95% CI 0.88–53.36; p = 0.066;Table 5;Figs. 4and5).
Predictors of tumor progression
| Predictive Factor | HR | 95% CI | p Value |
|---|---|---|---|
| Univariate analysis* | |||
| Location | |||
| All other locations | 1.00 | ||
| Parasellar/petroclival | 5.11 | 0.65–39.91 | 0.120 |
| History of radiotherapy | 3.73 | 1.00–13.94 | 0.050 |
| History of hydrocephalus | 1.19 | 1.00–1.41 | 0.056 |
| Any CN deficit from III to VI | 3.29 | 1.79–6.05 | <0.001 |
| Diplopia on presentation | 2.47 | 0.79–7.78 | 0.121 |
| Seizure | 7.64 | 1.53–38.04 | 0.013 |
| Tumor volume >14 cm3 | 6.86 | 0.88–53.36 | 0.066 |
| Decreasing maximal dose | 0.93 | 0.85–1.02 | 0.117 |
| Multivariate analysis | |||
| History of radiotherapy | 12.06 | 2.04–71.27 | 0.006 |
| Any CN deficit from III to VI | 3.78 | 1.91–7.45 | <0.001 |
| Tumor volume >14 cm3 | 6.86 | 0.88–53.36 | 0.066 |
Factors predictive of tumor progression (p < 0.20).
Graph of tumor-free progression in patients with and without a history of surgery.
Graph of tumor-free progression in patients stratified by tumor volume of 14 cm3.
Graph of tumor-free progression in patients with and without a history of radiotherapy.
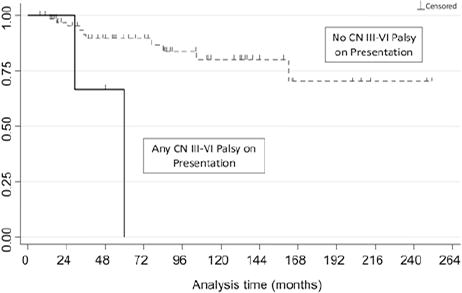
Graph of tumor-free progression in patients with and without a history of CN III, IV, V, or VI palsy on presentation.
Further Treatments Following SRS
During follow-up, 2 patients underwent fractionated radiation therapy for out-of-field tumor progression (3%), and 5 patients underwent resection for tumor progression (7%). All tumors resected after radiosurgery were confirmed to be WHO Grade I meningiomas. Three patients had evidence of radiological progression of ventriculomegaly, but none of these patients required a CSF diversion procedure.
Overall Outcome After SRS
Unfavorable outcome, defined as tumor progression and/or new or worsening decline in neurological function, was observed in 12 patients (18.8%), compared with 52 patients (81.2%) who had a favorable outcome. Of those with an unfavorable outcome, 7 patients (10.9%) exhibited both tumor progression and neurological decline.
单变量预测整体outco不利me (i.e., tumor growth and/or neurological decline) are detailed inTable 6. Statistically significant factors in univariate analysis for an unfavorable outcome included petroclival/ parasellar location, prior radiotherapy, prior surgery, any CN deficit from III to VI, diplopia on presentation, preexisting seizures, pre-GKRS edema, and decreasing maximal and peripheral dose (Table 6). Patients with a history of resection before radiosurgery were significantly more likely to have an unfavorable outcome in univariate analysis (OR = 2.37, 95% CI 1.08–5.21; p = 0.032), but prior resection was not an independent predictor of outcome. Youden indices did not provide a significant cutoff for the dichotomized continuous variable “tumor volume” that yielded the optimal discrimination of overall outcome.
Predictors of overall outcome
| Predictor of Unfavorable Outcome* | OR | 95% CI | p Value |
|---|---|---|---|
| Univariate analysis† | |||
| Location | |||
| All other locations | 1.00 | ||
| Parasellar/petroclival | 8.07 | 0.97–67.18 | 0.054 |
| History of radiotherapy | 5.44 | 0.95–31.36 | 0.058 |
| History of surgery | 2.37 | 1.08–5.21 | 0.032 |
| Any CN deficit from III to VI | 3.52 | 1.58–7.80 | 0.002 |
| Diplopia on presentation | 2.71 | 0.75–9.82 | 0.128 |
| Seizure | 10.20 | 0.84–123.56 | 0.068 |
| Pre-GKRS edema | 2.99 | 0.69–12.89 | 0.142 |
| Decreasing peripheral dose | 0.68 | 0.61–1.02 | 0.068 |
| Decreasing maximal dose | 0.85 | 0.74–0.97 | 0.019 |
| Multivariate analysis | |||
| History of radiotherapy | 3.39 | 1.11–10.39 | 0.033 |
| Any CN deficit from III to VI | 4.88 | 1.13–20.99 | 0.033 |
| Decreasing maximal dose | 0.78 | 0.66–0.93 | 0.006 |
Favorable outcome = tumor control and no new or worsening decline in neurological function.
Factors predictive of unfavorable outcome (p < 0.20).
In the multivariate analysis, the factors predictive of unfavorable outcome included history of prior radiation therapy (OR = 3.39, 95% CI 1.11–10.39; p = 0.033), presentation with any CN deficit from III to VI (OR = 4.88, 95% CI 1.13–20.99; p = 0.033), and decreasing maximal radiosurgical dose (OR = 0.78, 95% CI 0.66–0.93; p = 0.006). Becasue maximal dose was not completely linear and overall outcome also depended on patient and tumor characteristics, Youden indices did not identify an optimal breakpoint for maximal dose that was applicable to all tumors.
Discussion
Traditionally, meningiomas are treated with upfront surgery with the goal of complete resection.7,9,40,41,53Primary extirpation remains the gold standard of treatment for meningiomas. However, gross-total resection is often not possible. SRS has offered a viable alternative as well as an approach to achieve tumor control, especially for meningiomas that are challenging to resect such as those of the skull base.1,21,25,27,34,35,56Combinations of microsurgery and SRS may yield even greater local control for select meningiomas arising from the cranial base.11,17,23,29,33,37,44One such large study from the University of Pittsburgh with 972 patients, mostly with skull base meningiomas, reported actuarial tumor control rates of 93% at 5 years and 87% at 10 and 15 years.33However, the majority of meningioma SRS studies have not differentiated tumors by size, and many patient series exclude tumors of larger volume. Most radiosurgical series, in fact, include only small to moderately sized meningiomas under 8 cm3在总量(例如,平均不到diameter of 2.5 cm).
Stratifying meningiomas by size is expected to yield different GKRS planning and prognostic outcomes, especially in confined areas such as the skull base. A recent study by Oya and colleagues reported that initial meningioma diameters greater than 25 mm was a factor associated with a short time to progression (p = 0.0004) and a higher annual growth rate (p < 0.0001).42This finding confirms earlier multivariate analysis that linked lower rates of tumor control with higher tumor volume.29Other studies, including one from the University of Pittsburgh, have found that tumor volume greater than 8 cm3was the most important parameter associated with a worse prognosis for radiosurgery of benign meningiomas.8,15,16,20
From 1989 through 2012, our Gamma Knife center treated 75 patients with meningiomas at least 8 cm3in volume at initial planning (mean preradiosurgical tumor volume = 14.1 cm3). Forty percent of patients were treated with primary radiosurgery, and the remaining 60% were treated following resection. This division of primary radiosurgery and combination therapy patient populations was consistent with previous reports.8,11,17,23,29,37,44最后辐射后续(平均随访大调的ation 6.5 years), 84% displayed no change or a decrease in tumor volume on MRI, and 16% demonstrated an increase in volume. Our extended period of follow-up more accurately accounts for the known long-term natural history and recurrence rates of these Grade I meningiomas. Radiological progressionfree survival rates at 5 and 10 years were determined to be 89% and 77%, respectively. In the Cox multivariate analysis, the covariates associated with tumor progression included presentation with any CN deficit from III to VI, history of radiotherapy, and tumor volume greater than 14 cm3. These results in terms of tumor control for large meningiomas are promising, and at least for skull base meningiomas, the results appear to challenge traditional dogma relegating radiosurgery only to small or moderately sized tumors. When prior resection is undertaken, meningioma reduction to a volume of 14 cm3or less appears to result in a reasonable target volume for single-session radiosurgery.
Our results appear to be comparable with other studies of radiosurgery for large meningiomas.8,16,20,45,52Two small series with a mean follow-up of approximately 30 months reported 100% tumor control of all meningiomas with volumes greater than 10 cm3.45,52Another study with longer follow-up by Haselsberger et al. similarly found excellent tumor control with staged GKRS for large benign meningiomas.20Of their 20 patients with treatment volumes between 5.4 and 43 cm3(median 19 cm3), tumor control was achieved in 90% of cases. The 2 patients who initially experienced tumor progression in areas outside of the planning target volumes ultimately received additional radiosurgical procedures that resulted in subsequent tumor volume control. Ganz et al. reported 100% tumor control in their 97 patients with meningiomas greater than 10 cm3and a mean follow-up of 4.5 years.16Tumor regression was observed in 28% of tumors at last radiological follow-up. An institutional review of large-volume benign meningiomas at the Mayo Clinic reported tumor control rates of 99% at 3 years and 92% at 7 years after radiosurgery.8The mean tumor margin dose was 15.1 Gy, and the mean preradiosurgical tumor volume was 17.5 cm3. These investigators found no factors to be associated with tumor growth after radiosurgery. Iwai et al. presented 7 cases of large petroclival or cavernous sinus meningiomas treated with staged GKRS.24Six patients (86%) did not have any tumor growth on last imaging. Unfortunately, the duration of their follow-up period (mean 39 months) limits the significance of these results, given the slow growth pattern of meningiomas and long-term mechanism of GKRS.
At last clinical follow-up, 83% of patients in this current series demonstrated improvement or no change in their neurological condition and 17% showed deterioration. Also, 4 patients had new or worsened peritumoral edema following radiosurgery. In multivariate analysis, history of surgery, presentation with any CN deficit from III to VI, and decreasing maximal dose were factors predictive of new or worsening decline in neurological condition. Tumor progression was present in 64% of patients who experienced new or worsening neurological decline. Unfavorable outcome (i.e., tumor progression or new or worsening decline in neurological function) was observed in 19% of patients. In the multivariate analysis, history of radiotherapy, presentation with any CN deficit from III to VI, and decreasing maximal dose were predictive of unfavorable outcome. Our clinical results are comparable to similar patient populations.8,16,20,45Pendl et al. reported 88% clinical improvement or stability and 2 patients with new CN deficits (facial and optic nerve) at last clinical follow-up (mean of 28 months).45Haselsberger et al. reported that 45% of patients saw clinical improvement and 55% remained clinically stable at last follow-up (median of 7.5 years).20Commonly reported complications included transient nausea and emesis immediately posttreatment, peritumoral edema that often resolves within the first 6 months, headaches, and CN deficits. Three of the 97 patients in the study by Ganz et al. suffered adverse radiation effect (i.e., post-SRS edema), all of which resolved completely within the follow-up period.16Bledsoe et al. reported a complication rate of 23% after radiosurgery.8他们的并发症,为了减少frequency, included seizures, hemiparesis, trigeminal injury, headaches, diplopia, cerebral infarction, ataxia, and hearing loss. When analyzing their series by tumor location, they noted a statistically significant difference in complication rates between patients with supratentorial tumors and those with skull base tumors (44% vs 18%, respectively). This data further supports reasonably safe management of large-volume skull base meningiomas with radiosurgery.
Radiological and clinical outcomes from our and other presented series of large meningiomas are similar to those obtained in series of smaller meningiomas of the skull base.11,17,23,29,33,37,44We surmise that these results are similar due to advances in radiosurgical technology that have focused on more accurate targeting and limiting unnecessary radiation to nearby viable tissue. The goal of GKRS for large-sized meningiomas is similar to that of smaller lesions, which is to prevent tumor progression without incurring radiosurgical morbidity by reducing the margin dose. However, radiosurgical planning of larger tumors requires particular attention to tumor location and surrounding structures. Optimal planning requires consideration of achieving optimal dose gradients and varying them when prudent. For example, for a large skull base meningioma, the dose gradient in the direction of the brainstem with critical neurological structures may need to be steeper than that to the petrous bone, with fewer at-risk structures.
Typically, large meningiomas cause local mass effect to which the brain adapts and may even continue to function normally as growth gradually occurs over many years. This means surrounding structures may still be viable but are closely approximated to the tumor, thereby increasing the difficult of complete resection. Over the last few decades, improved precision of radiosurgical planning has helped to minimize radiation overlap. Highly conformal dose planning has permitted effective coverage of irregularly shaped tumors and even dural tails to be included within the prescription isodose line. DiBiase et al. noted that inclusion of the dural tail in the treatment volume rendered a significantly higher 5-year disease-free survival score than not including the tail (96% vs 78%, respectively).13Furthermore, the trend of reduced marginal doses to around 12 Gy has proven just as efficacious for tumor control as higher doses, while limiting radiation dosage to nearby neurovascular structures.22,28,46Ganz et al. recommended that the marginal dose be kept at 12 Gy and only reduced if it was necessary to protect normal tissue.16
Hypofractionated or multisession radiosurgical procedures also offers steep radiation falloff to protect adjacent tissue from radiation-induced injury.24,43,45Multisession radiosurgery may allow for effective management of larger skull base meningiomas. Even when benign meningiomas are discovered at larger sizes, their lack of invasion and clear visualization on neuroimaging permit complete radiation coverage of the tumor cells.
Our study is one of the largest radiosurgical series of large skull base meningiomas to date. However, this study remains limited by its retrospective nature and by institutional selection and treatment biases. Additionally, in this study we sought to determine the outcomes following planned single-session radiosurgery, and thus we did not include patients with multisession treatment plans or fractionated radiosurgery. The treatment period of this study also includes over two decades of treatment, and during this period, GKRS technology, radiosurgical technique, and neuroimaging have generally improved. Only a small set of select patients were only evaluated by pre- and post-treatment CT scans. Contouring of the tumor volume is also a potential source of bias. We are unable to reliably determine how refinements in GKRS units, treatment planning, neuroimaging, and targeting strategies may have altered our outcomes. Additionally, a number of posttreatment effects of frame-based radiosurgery such as headache, pin site infection, and fatigue were not routinely captured as part of this study; unfortunately, we do not have sufficient data to fully account for these types of complications. Additional neuropsychiatric and electrophysiological testing would be beneficial to further define potential subtle complications. Finally, it is not clear whether these results for large skull base meningiomas are generalizable to large meningiomas involving other intracranial locations. In particular, large parasagittal and parafalcine meningiomas that are in close proximity to large venous structures have been previously shown to have greater risk of symptomatic postradiosurgical peritumoral edema.14Further assessment of large patient cohorts may be necessary to fully define the edema risk in skull base lesions in close proximity to key deep and large venous structures
Conclusions
Stereotactic radiosurgery affords a reasonable rate of tumor control for large skull base meningiomas, and it accomplishes this with an acceptably low incidence of neurological deterioration. Surgery may be the preferred treatment option for lesions larger than 8 cm3(an approximate tumor diameter of 2.5 cm) when patients have growing and symptomatic lesions (e.g., those presenting with any CN deficit from III to VI). However, in cases of enlarging asymptomatic lesions, recurrent or residual lesions following resection, significant patient comorbidities, and patient preference, SRS demonstrates reasonable results for large meningiomas.
Author Contributions
Conception and design: Sheehan, Starke. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Statistical analysis: Starke. Administrative/technical/material support: Sheehan. Study supervision: Sheehan, Starke.
References
-
1 ↑
AichholzerM,,BertalanffyA,,DietrichW,,RoesslerK,,PfistererW,&UngersboeckK,et al.:Gamma knife radiosurgery of skull base meningiomas.Acta Neurochir (Wien)142:647–653,2000
-
3 ↑
Al-MeftyO,,FoxJL,&SmithRR:Petrosal approach for petroclival meningiomas.开云体育app官方网站下载入口22:510–517,1988
-
5 ↑
ArnautovićKI,,Al-MeftyO,&HusainM:Ventral foramen magnum meninigiomas.J Neurosurg92:1 Suppl71–80,2000
-
6 ↑
BambakidisNC,,KakarlaUK,,KimLJ,,NakajiP,,PorterRW,&DaspitCP,et al.:Evolution of surgical approaches in the treatment of petroclival meningiomas: a retrospective review.开云体育app官方网站下载入口61:5 Suppl 2202–211,2007
-
7 ↑
BassiouniH,,AsgariS,&StolkeD:Tuberculum sellae meningiomas: functional outcome in a consecutive series treated microsurgically.Surg Neurol66:37–45,2006
-
8 ↑
BledsoeJM,,LinkMJ,,StaffordSL,,ParkPJ,&PollockBE:Radiosurgery for large-volume (> 10 cm3) benign meningiomas.J Neurosurg112:951–956,2010
-
10 ↑
CouldwellWT,,KanP,,LiuJK,&ApfelbaumRI:Decompression of cavernous sinus meningioma for preservation and improvement of cranial nerve function. Technical note.J Neurosurg105:148–152,2006
-
11 ↑
DavidsonL,,FishbackD,,RussinJJ,,WeissMH,,YuC,&PagniniPG,et al.:Postoperative Gamma Knife surgery for benign meningiomas of the cranial base.Neurosurg Focus23:4E6,2007
-
12 ↑
De SallesAAF,&GorgulhoAA,Radiosurgery for arteriovenous malformations.De SallesAAF,,GorgulhoA,&AgazaryanN,et al.:Shaped Beam Radiosurgery: State of the ArtBerlin,Springer-Verlag,2011.77–88
-
13 ↑
DiBiaseSJ,,KwokY,,YovinoS,,ArenaC,,NaqviS,&TempleR,et al.:Factors predicting local tumor control after gamma knife stereotactic radiosurgery for benign intracranial meningiomas.Int J Radiat Oncol Biol Phys60:1515–1519,2004
-
14 ↑
DingD,,XuZ,,McNeillIT,,YenCP,&SheehanJP:Radiosurgery for parasagittal and parafalcine meningiomas.J Neurosurg119:871–877,2013
-
15 ↑
FlanneryTJ,,KanoH,,LunsfordLD,,SirinS,,TormentiM,&NiranjanA,et al.:长期的合同rol of petroclival meningiomas through radiosurgery.J Neurosurg112:957–964,2010
-
16 ↑
GanzJC,,RedaWA,&AbdelkarimK:Gamma Knife surgery of large meningiomas: early response to treatment.Acta Neurochir (Wien)151:1–8,2009
-
17 ↑
GoldsmithBJ,,WaraWM,,WilsonCB,&LarsonDA:Postoperative irradiation for subtotally resected meningiomas. A retrospective analysis of 140 patients treated from 1967 to 1990.J Neurosurg80:195–201,1994
-
18 ↑
González-DarderJM,,Pesudo-MartínezJV,,Feliu-TatayR,&Borrás-MorenoJM:[Neurosurgical treatment of acoustic neuromas without indication for radiosurgery].Neurocirugia (Astur)15:439–446,2004.(Span)
-
19 ↑
HasegawaT,,KidaY,,YoshimotoM,,KoikeJ,,IizukaH,&IshiiD:Long-term outcomes of Gamma Knife surgery for cavernous sinus meningioma.J Neurosurg107:745–751,2007
-
20 ↑
HaselsbergerK,,MaierT,,DominikusK,,HollE,,KurschelS,&Ofner-KopeinigP,et al.:Staged gamma knife radiosurgery for large critically located benign meningiomas: evaluation of a series comprising 20 patients.J Neurol Neurosurg Psychiatry80:1172–1175,2009
-
21 ↑
IgakiH,,MaruyamaK,,KogaT,,MurakamiN,,TagoM,&TeraharaA,et al.:Stereotactic radiosurgery for skull base meningioma.神经医学Chir(东京)49:456–461,2009
-
22 ↑
IwaiY,,YamanakaK,&IkedaH:Gamma Knife radiosurgery for skull base meningioma: long-term results of low-dose treatment.J Neurosurg109:804–810,2008
-
23 ↑
IwaiY,,YamanakaK,&NakajimaH:The treatment of skull base meningiomas—combining surgery and radiosurgery.J Clin Neurosci8:528–533,2001
-
24 ↑
IwaiY,,YamanakaK,&NakajimaH:Two-staged gamma knife radiosurgery for the treatment of large petroclival and cavernous sinus meningiomas.Surg Neurol56:308–314,2001
-
25 ↑
IwaiY,,YamanakaK,,YasuiT,,KomiyamaM,,NishikawaM,&NakajimaH,et al.:Gamma knife surgery for skull base meningiomas. The effectiveness of low-dose treatment.Surg Neurol52:40–45,1999
-
26 ↑
JungYJ,,LymYS,,LeeJI,,NamDH,,ParkK,&KimJH:Gamma knife radiosurgery for brain metastases in patients harboring four or more lesions: survival and prognostic factors.J Korean Neurosurg Soc36:206–212,2004
-
27 ↑
KollováA,,LiscákR,,NovotnýJJr,,VladykaV,,SimonováG,&JanouskováL:Gamma Knife surgery for benign meningioma.J Neurosurg107:325–336,2007
-
28 ↑
KondziolkaD,,FlickingerJC,&LunsfordLD:The principles of skull base radiosurgery.Neurosurg Focus24:5E11,2008
-
29 ↑
KondziolkaD,,FlickingerJC,&PerezB:Judicious resection and/or radiosurgery for parasagittal meningiomas: outcomes from a multicenter review.开云体育app官方网站下载入口43:405–414,1998
-
30
KondziolkaD,&LunsfordLD:Radiosurgery of meningiomas.Neurosurg Clin N Am3:219–230,1992
-
31
KondziolkaD,,LunsfordLD,&FlickingerJC,Stereotactic radiosurgery of meningioma.LunsfordLD,,KondziolkaD,&FlickingerJC:Gamma Knife Brain SurgeryNew York,Karger,1998.104–113
-
32
KondziolkaD,,LunsfordLD,,LinskeyME,&FlickingerJC,Skull base radiosurgery.AlexanderEIII,,LoefflerJS,&LunsfordLD:Stereotactic RadiosurgeryNew York,McGraw Hill,1993.175–188
-
33 ↑
KondziolkaD,,MathieuD,,LunsfordLD,,MartinJJ,,MadhokR,&NiranjanA,et al.:Radiosurgery as definitive management of intracranial meningiomas.开云体育app官方网站下载入口62:53–60,2008
-
34 ↑
KreilW,,LugginJ,,FuchsI,,WeiglV,,EustacchioS,&PapaefthymiouG:Long term experience of gamma knife radiosurgery for benign skull base meningiomas.J Neurol Neurosurg Psychiatry76:1425–1430,2005
-
35 ↑
LeeJY,,NiranjanA,,McInerneyJ,,KondziolkaD,,FlickingerJC,&LunsfordLD:Stereotactic radiosurgery providing longterm tumor control of cavernous sinus meningiomas.J Neurosurg97:65–72,2002
-
36 ↑
MathiesenT,,GerlichA,,KihlströmL,,SvenssonM,&Bagger-SjöbäckD:Effects of using combined transpetrosal surgical approaches to treat petroclival meningiomas.开云体育app官方网站下载入口60:982–992,2007
-
37 ↑
MetellusP,,RegisJ,,MuraccioleX,,FuentesS,,DufourH,&NanniI,et al.:Evaluation of fractionated radiotherapy and gamma knife radiosurgery in cavernous sinus meningiomas: treatment strategy.开云体育app官方网站下载入口57:873–886,2005
-
38 ↑
MinnitiG,,AmichettiM,&EnriciRM:Radiotherapy and radiosurgery for benign skull base meningiomas.Radiat Oncol4:42,2009
-
39 ↑
NicolatoA,,ForoniR,,AlessandriniF,,MalutaS,,BricoloA,&GerosaM:The role of Gamma Knife radiosurgery in the management of cavernous sinus meningiomas.Int J Radiat Oncol Biol Phys53:992–1000,2002
-
40 ↑
O'SullivanMG,,van LoverenHR,&TewJMJr:The surgical resectability of meningiomas of the cavernous sinus.开云体育app官方网站下载入口40:238–247,1997
-
41 ↑
OtaniN,,MuroiC,,YanoH,,KhanN,,PangaluA,&YonekawaY:Surgical management of tuberculum sellae meningioma: role of selective extradural anterior clinoidectomy.Br J Neurosurg20:129–138,2006
-
42 ↑
OyaS,,KimSH,,SadeB,&LeeJH:The natural history of intracranial meningiomas.J Neurosurg114:1250–1256,2011
-
43 ↑
PatilCG,,HoangS,,BorchersDJIII,,SakamotoG,,SoltysSG,&GibbsIC,et al.:Predictors of peritumoral edema after stereotactic radiosurgery of supratentorial meningiomas.开云体育app官方网站下载入口63:435442,2008
-
44 ↑
PendlG,,SchröttnerO,,EustacchioS,,GanzJC,&FeichtingerK:Cavernous sinus meningiomas—what is the strategy: upfront or adjuvant gamma knife surgery?.Stereotact Funct Neurosurg70:Suppl 133–40,1998
-
45 ↑
PendlG,,UngerF,,PapaefthymiouG,&EustacchioS:上演radiosurgical treatment for large benign cerebral lesions.J Neurosurg93 Suppl 3:107–112,2000
-
46 ↑
SheehanJP,,WilliamsBJ,&YenCP:Stereotactic radiosurgery for WHO grade I meningiomas.J Neurooncol99:407–416,2010
-
47 ↑
SnellJW,,SheehanJ,,StroilaM,&SteinerL:Assessment of imaging studies used with radiosurgery: a volumetric algorithm and an estimation of its error. Technical note.J Neurosurg104:157–162,2006
-
48 ↑
StaffordSL,,PollockBE,,FooteRL,,LinkMJ,,GormanDA,&SchombergPJ,et al.:Meningioma radiosurgery: tumor control, outcomes, and complications among 190 consecutive patients.开云体育app官方网站下载入口49:1029–1038,2001
-
49 ↑
StarkeRM,,WilliamsBJ,,HilesC,,NguyenJH,,ElsharkawyMY,&SheehanJP:Gamma knife surgery for skull base meningiomas.J Neurosurg116:588–597,2012
-
50 ↑
SubachBR,,LunsfordLD,,KondziolkaD,,MaitzAH,&FlickingerJC:Management of petroclival meningiomas by stereotactic radiosurgery.开云体育app官方网站下载入口42:437–445,1998
-
51 ↑
TakanashiM,,FukuokaS,,HojyoA,,SasakiT,,NakagawaraJ,&NakamuraH:Gamma knife radiosurgery for skull-base meningiomas.Prog Neurol Surg22:96–111,2009
-
52 ↑
TunizF,,SoltysSG,,ChoiCY,,ChangSD,,GibbsIC,&FischbeinNJ,et al.:Multisession cyberknife stereotactic radiosurgery of large, benign cranial base tumors: preliminary study.开云体育app官方网站下载入口65:898–907,2009
-
53 ↑
VossNF,,VrionisFD,,HeilmanCB,&RobertsonJH:Meningiomas of the cerebellopontine angle.Surg Neurol53:439–447,2000
-
54 ↑
WilliamsBJ,,YenCP,,StarkeRM,,BasinaB,,NguyenJ,&RaineyJ,et al.:Gamma Knife surgery for parasellar meningiomas: long-term results including complications, predictive factors, and progression-free survival.J Neurosurg114:1571–1577,2011
-
55 ↑
YaşargilMG:Meningiomas.Microneurosurgery: Microneurosurgery of CNS TumorsNew York,蒂米医学出版商,1996.IV-B:134–165
-
56 ↑
ZachenhoferI,,WolfsbergerS,,AichholzerM,,BertalanffyA,,RoesslerK,&KitzK,et al.:Gamma-knife radiosurgery for cranial base meningiomas: experience of tumor control, clinical course, and morbidity in a follow-up of more than 8 years.开云体育app官方网站下载入口58:28–36,2006