

Thelateral posterior choroidal artery (LPChA) was first described by Beevor1in 1909 as a group of branches from the posterior cerebral artery (PCA) that supply the central part of thelateral ventricle. Subsequently, in the 1950s, Millen and Woollam2and Hudson3conducted comparative studies to describe the vascular pattern of the choroid plexus and proposed the subdivision of choroidal arteries into posterior inferior, posterior medial, and posterior lateral segments. In 1960, Galloway and Greitz4further studied the medial and lateral choroidal arteries, introducing angiographic methods. In 1980, Fujii, Lenkey, and Rhoton5completed the first detailed microsurgical anatomy study of the choroidal arteries and classified the LPChA into cisternal and plexal segments; as concluded by Rhoton, the surgical management of ventricular tumors involving the LPChA remains a distinct challenge for neurosurgeons, because the LPChA not only supplies the choroid plexus but also may vascularize adjacent critical neurovascular structures such as the parahippocampus, visual pathways, and pulvinar ofthalamus. Therefore, understanding the anatomical features of the LPChA is of utmost importance for the neurosurgeon dealing with intraventricular lesions.
Since the pioneering investigation of Rhoton, very few studies have focused on the LPChA,6–9and there is still little knowledge regarding relevant surgical landmarks, anatomical variations and patterns, the exact relationship with theanterior choroidal artery(AChA), and the extent of nonchoroidal vascular supply; also, importantly, there has not been an updated description of the LPChA in the context of different surgical routes to the choroid plexus, including the transsylvian trans–limen insulae, lateral transtemporal, and transparietal transcortical approaches.
In this study, we aim to delineate the microsurgical anatomy of the LPChA and its surgical implications by using anatomical microdissections. We describe the anatomical trajectory and variations of the LPChA, emphasizing its anatomical segments and their relationship with adjacent neurovascular structures, and discuss the surgical implications when approaching the choroid plexus via different routes.
开云体育世界杯赔率
Twelve colored silicone–injected postmortem human head specimens that had been lightly fixed and preserved in a 95% ethyl alcohol solution were prepared for dissection. Anatomical dissection was performed in all heads by using a frontotemporal craniotomy for the transsylvian and lateral transtemporal approaches, and using a parietal craniotomy for the transparietal transcortical and contralateral posterior interhemispheric transfalcine transprecuneus approaches. The origin, diameter, trunk, course, segment, length, and anastomosis of the LPChA were investigated, and its spatial relationships with the AChA, fimbria, crus offornix, and pulvinar were carefully inspected. The diameter of the AChA and LPChA and the distance between them at theinferior choroidal pointwere measured with digital micrometer calipers. The LPChA was classified into normal, hypoplastic (defined as less than half of the diameter of the AChA), and hyperplastic (defined as larger than the diameter of the AChA). The patterns of the LPChA were divided into 3 types according to its location in relation to thechoroidal fissureand the number of trunks. The microsurgical anatomy and surgical landmarks of each approach to the LPChA were also examined thoroughly. Once the surgical approaches were completed, the medial temporal lobes were dissected to study the architecture of the neurovascular structures around the LPChA.
To provide maximal visualization, a ×3- to ×40-magnification microscope (Haag-Streit Surgical); 0° and 30° rod–lens endoscopes attached to 4K cameras (4 mm, 18 cm, Hopkins II; Karl Storz); and a high-definition camera (Canon) were used in all steps. All data were analyzed using SPSS 26.0 (IBM Corp.). Values are expressed as the mean ± SD, and Pearson’s correlation coefficient was calculated to evaluate a possible correlation in continuous variables.
Results
Microsurgical Anatomy of the LPChA
Origin
The LPChA was identified in 23 hemispheres (96%), and the PCA served as its origin in all of them. In 6 hemispheres (26%) the LPChAs originated from the anterior segment of the P2 (P2A), and in 14 hemispheres (61%) they arose from the posterior segment (P2P). In only 1 hemisphere (4%) it originated from P3; in 1 hemisphere (4%) it originated from the parieto-occipital artery, and in 1 hemisphere (4%) it originated from the middle inferior temporal artery. In no case was there an anomalous origin of the artery from theinternal carotid artery(ICA) or posterior communicating artery (Figs. 1and2,Table 1). The LPChA was categorized based on its diameter into the following groups: normal (53%); hypoplastic (30%); hyperplastic (13%); and absent (4%). The diameter of the LPChA was inversely correlated to the diameter of the AChA according to Pearson correlation analyses (R = −0.459; p < 0.05)4(Fig. 3C–F).

Anatomical views of the LPChA in the temporal horn and atrium.A:The left frontal and parietal lobes have been removed to reveal the LPChA from an anterolateral view.B:Enlargement of panel A shows several trunks of LPChA with a classic C-shaped trajectory, curving forward and laterally around the parahippocampal gyrus in the ambient cistern to enter the choroidal fissure, running medially along the choroid plexus.C:The choroid plexus and its vessels have been isolated and removed on the same specimen as seen in panels A and B. The vascular network is formed by the AChA and 3 LPChA trunks.D:The right superior temporal gyrus and parietal lobules have been removed in a different specimen to reveal the atrium and LPChA from a posterolateral view. The LPChA runs medially along the choroid plexus.E:Enlargement of thedashed boxmarked in panel D. The forniceal segment of the LPChA runs along the superior surface of the fimbria along the medial border of the choroid plexus, whereas the AChA gives off brush-like branches along the lateral border of the choroid plexus. Anastomoses were observed between LPChA and AChA at the atrium.F:Lateral view of the LPChA in the temporal horn of the same specimen. The LPChA enters the choroidal fissure approximately 8 mm posterior to the AChA.G:Removal of the hippocampus and fornix (crus and fimbria) reveals the whole course of the LPChA with 2 trunks. The superior trunk runs above the fimbria and crus of fornix to end at the lateral pulvinar, whereas the inferior LPChA trunk approaches the fimbrio-dentate sulcus and runs under the fimbria without entering the choroidal fissure, to then stop at the medial pulvinar. The MPChA is located in the quadrigeminal cistern to enter the roof of the third ventricle.H:The vascular network of the choroid plexus in another specimen is composed of the AChA and 2 LPChA trunks divided into 3 segments: 1) cisternal; 2) forniceal; and 3) pulvinar. Panels A–H copyright Juan Carlos Fernandez-Miranda. Published with permission.I:Artistic illustration of the LPChA route from the posterior view. The LPChA originates from the PCA and runs medially to the AChA in the choroid plexus and stops in the pulvinar. Artists (panel I): David Rini and Diane Abeloff. Copyright Aaron Cohen-Gadol. Published with permission fromThe Neurosurgical Atlasby Aaron Cohen-Gadol. A. = artery; A.Ch.A. = anterior choroidal artery; Atr. V. = atrial vein; BA = basilar artery; Calc. = calcarine; Call. = callosal; Chor. = choroid, choroidal; Cing. = cingulate; CN = cranial nerve; Coll. = colliculus; Comm. = commissure; Hippo. = hippocampal; Inf. = inferior; Lat. = lateral; L.P.Ch.A. = lateral posterior choroidal artery; Marg. = marginal; Med. = medial; M.P.Ch.A. = medial posterior choroidal artery; Occip. = occipital; Peri. Call. = pericallosal; Plex. = plexus; Post. = posterior; Prox. Bifurc. = proximal bifurcation; Pt. = pituitary; Sulc. = sulcus; Sup. = superior; Temp. = temporal; V. = vein. Figure is available in color online only.
Anatomical views of the LPChA in the temporal lobe.A:The left hemisphere has been removed with the exception of the parahippocampal gyrus. The AChA arises from the ICA to enter the lateral ventricle at the inferior choroidal point, whereas the LPChA arises from the PCA and enters the lateral ventricle posterior to the inferior choroidal point. Both of them participate in the blood supply of the choroid plexus.B:The optic tract has been elevated to display the contents of the crural cistern and the relationships of the AChA, LPChA, inferior choroidal vein, and basal vein in the region of the inferior choroidal point. The LPChA ramifies into several branches at the beginning of the fimbria segment to supply the choroid plexus.C:Superior view of LPChA in another specimen; the LPChA enters the lateral ventricle in the posterior limit of the uncus, posterior to the AChA. After it passes the fimbria, a confluence of LPChA and AChA is observed. The MPChA runs in the medial side of the LPChA.D:Internal view of the same specimen, which displays 2 trunks of LPChA: the superior trunk originated from P2A and enters the anterior choroidal fissure between the fimbria and LGB, whereas the inferior LPChA trunk originated from P2P and enters the posterior choroidal fissure between the pulvinar and the crus of fornix.E:Medial–superior view of the relationship of LPChA with adjacent neurovascular structures in another specimen. The PCA has been removed. The LPChA originates from the PCA and runs as a C-shaped trajectory curving forward and laterally around the parahippocampal gyrus in the ambient cistern to enter the choroidal fissure posterior to the inferior choroidal point.F:The basal vein system was removed in the inferior choroidal point to reveal the distance and anastomosis between the AChA and LPChA. A. = artery; A.Ch.A. = anterior choroidal artery; Ant. = anterior; Cer. = cerebral; Chor. = choroid, choroidal; Clin. = clinoid; CN = cranial nerve; Giac. = Giacomini; Hippo. = hippocampal; Inf. = inferior; Int. = internal; L.P.Ch.A. = lateral posterior choroidal artery; Mid. = middle; M.P.Ch.A. = medial posterior choroidal artery; Parahippo. = parahippocampal; Plex. = plexus; Post. = posterior; Proc. = process; Temp. = temporal; Uncin. = uncinate; V. = vein. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Microsurgical anatomy of the LPChA in 24 human cadaveric hemispheres
| Characteristic of LPChA | Value |
|---|---|
| Present | |
| Hypoplastic | 7 (30%) |
| Normal | 13 (57%) |
| Hyperplastic | 3 (13%) |
| Absent | 1 (4%) |
| Origin | |
| P2A | 6 (26%) |
| P2P | 14 (61%) |
| P3 | 1 (4%) |
| POA | 1 (4%) |
| MITA | 1 (4%) |
| Trunk | |
| Single | 7 (30%) |
| Double | 14 (61%) |
| ≥Triple | 2 (9%) |
| Course | |
| C-shaped | 17 (74%) |
| Serpentine | 6 (26%) |
| Segment | Length (mm) | Origin | Destination | Branches (%) |
|---|---|---|---|---|
| Cisternal | 10.6 ± 2.5 | PCA | Anterior choroidal fissure | Parahippocampus (73%); hippocampus (49%); LGB (12%) |
| Forniceal | 28.7 ± 6.8 | Anterior choroidal fissure | Posterior choroidal fissure | Choroid plexus (95%); thalamus (35%) |
| Pulvinar | 5.9 ± 2.2 | Posterior choroidal fissure | Pulvinar | Choroid plexus (81%) |
MITA = middle inferior temporal artery; POA = parieto-occipital artery.
Angiography and anatomical hypoplasty of the LPChA.A and B:Two cases of the lateral view from digital subtraction angiography with selective right common carotid injection to display the course of the LPChA, which arises from the PCA and joins with the AChA to supply the choroid plexus. Notice that panel B shows a fetal PCA.C:Medial view of the left hippocampus shows tenuous LPChA arising from the PCA and crossing the surface of the fimbria to join the choroid plexus.D:The choroid plexus and its vessels have been isolated and removed on the same specimen as in panel C; note the different calibers between the AChA and LPChA.E:Medial–superior view of the left temporal lobe in a different specimen. Two hypoplastic LPChAs run along the medial border of the choroid plexus, which is mostly supplied by a large AChA.F:脉络丛血管网络的隔离d from the specimen in panel E; the diameter of the LPChA is inversely correlated to the diameter of the AChA. A. = artery; A.Ch.A. = anterior choroidal artery; Chor. = choroid, choroidal; Dent. = dentate; Hippo. = hippocampal; Inf. = inferior; L.P.Ch.A. = lateral posterior choroidal artery; Mid. = middle; M.P.Ch.A. = medial posterior choroidal artery; Ophthal. = ophthalmic; Parahippo. = parahippocampal; P.Co.A. = posterior communicating artery; Plex. = plexus; Post = posterior; Sup. = superior; Temp. = temporal; V. = vein. Panels C–F copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Trunk
The LPChA was observed as a double trunk (inferior and superior) most frequently (61%), as a single trunk in 30%, and as 3 or more trunks in 9%. In hemispheres with a double trunk, 36% arose as a large common trunk from the PCA with bifurcation later, whereas 64% originated as independent trunks from the PCA. The superior LPChA trunk typically traveled along theambient cisternto enter into the choroidal fissure and supply the choroid plexus and then ran above the fimbria and crus of fornix to end at the lateral pulvinar. The inferior LPChA trunk most frequently approached the fimbrio-dentate sulcus running under the fimbria, rarely entering the choroidal fissure, to then stop at the medial pulvinar. Anastomoses were observed between these 2 trunks in 6 of 14 hemispheres (43%) (Figs. 1–3,Table 1).
Course
In 74% of hemispheres, the LPChA had a classic C-shaped trajectory, curving forward and laterally around the parahippocampal gyrus in the ambient cistern to enter the choroidal fissure at a distance of 8.2 ± 5.7 mm posterior to the AChA entrance at the inferior choroidal point. In 26% of hemispheres, the LPChA had an atypical serpentine-shaped trajectory (Figs. 1–3,Table 1).
Segmentation
The LPChA was divided into 3 segments according to its course and vascular territories: cisternal, forniceal, and pulvinar segments (Fig. 1,Table 1). Segments are described as follows.
1) Cisternal segment: this first segment runs in the ambient cistern, lateral to the cerebral crus, starting from its PCA origin and ending at the choroidal fissure. This segment was 10.6 ± 2.5 mm long and gave off branches to the parahippocampus (73%),hippocampus(49%), and lateral geniculate bodies (LGBs) (12%). If there were double trunks, the inferior trunk always stood inferoposterior to the superior trunk.
2) Forniceal segment: this segment starts at the anterior choroidal fissure, 8.2 ± 5.7 mm posterior to the AChA entrance at the inferior choroidal point, and then enters thetemporal horn在脉络丛的内侧边缘along the fimbria. When double trunks are present, the superior one runs as described above, and the inferior one courses along the fimbrio-dentate sulcus. This segment terminated at the posterior level of the choroidal fissure, between the pulvinar and the crus of fornix, and the length was 28.7 ± 6.8 mm. Along this segment, several branches were observed entering the choroid plexus with high frequency (95%).
3) Pulvinar segment: this last segment starts at the posterior choroidal fissure and terminates in the pulvinar in the form of perforating vessels on its surface. The length of this segment was 5.9 ± 2.2 mm.
LPChA Patterns
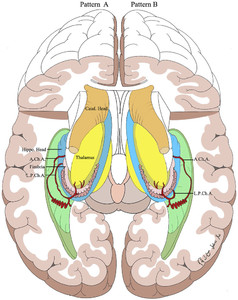
The LPChA was divided into 3 patterns according to the entrance of the LPChA in the choroidal fissure (anterior or posterior) and the number of trunks (Fig. 4).
Artistic illustration of the microsurgical patterns of the LPChA. The left side shows pattern A, where the LPChA enters the anterior choroidal fissure, between the fimbria and LGB; the right side shows pattern B, where the vessel enters the posterior choroidal fissure, between the crus of fornix and the pulvinar. A.Ch.A. = anterior choroidal artery; Caud. = caudate; Hippo. = hippocampal; L.P.Ch.A. = lateral posterior choroidal artery. Artist: Yuanzhi Xu. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Pattern A
The LPChA entered the anterior choroidal fissure, between the fimbria andLGB. Eighteen hemispheres (78%) presented this pattern in our study. Pattern A can be subdivided into 2 groups: A1 (single trunk, 6 hemispheres; 26%) and A2 (2 or more trunks, 12 hemispheres; 52%). This subdivision is relevant because in cases of a single trunk (A1), injury to the LPChA will probably cause a stroke in related territories, whereas in cases of multiple trunks this will be less likely (Fig. 5).
Pattern A of the LPChA: anatomical and artistic illustrations.A:Artistic illustration of pattern A. The left side shows pattern A1, where a single trunk enters the anterior choroidal fissure running above the fimbria. The right side shows pattern A2, which presents as multiple trunks, one of which serves as the superior trunk and enters the anterior choroidal fissure, whereas the inferior trunk runs under the fornix and toward the pulvinar. Artist: Yuanzhi Xu.B:The left parietal, occipital, and temporal lobes have been removed to reveal the LPChA trajectory.C:Enlargement of thedashed boxmarked in panel B. The LPChA enters the anterior choroidal fissure between the superior surface of the fimbria and LGB.D:The pulvinar has been elevated to show the origin of the LPChA from the PCA in the ambient cistern.E:Medial–superior view of the hippocampus in the same specimen. The LPChA bifurcates into 2 trunks; one serves as the superior trunk and enters the anterior choroidal fissure, whereas the inferior trunk runs along the fimbrio-dentate sulcus without entering the choroidal fissure to end at the medial pulvinar.F:Medial–superior view of the left hippocampus in another specimen. The LPChA presents as pattern A1, which consists of a single trunk entering the anterior choroidal fissure.G:Medial–superior view of the right hippocampus in another specimen, showing another example of pattern A1. A. = artery; A.Ch.A. = anterior choroidal artery; Amyg. = amygdala; Ant. = anterior; Calc. = calcarine; Chor. = choroid, choroidal; Cing. = cingulate; Comm. = commissure; Corp. Call. = corpus callosum; Fiss. = fissure; Hippo. = hippocampal; Inf. = inferior; Lat. = lateral; Lat. Geni. Body = lateral geniculate body; L.P.Ch.A. = lateral posterior choroidal artery; MCA = middle cerebral artery; Mid. = middle; Occip. = occipital; Plex. = plexus; Post. = posterior; Prox. Bifurc. = proximal bifurcation; Splen. = splenium; Temp. = temporal; V. = vein; Vent. = ventricle.Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Pattern B
The LPChA entered the posterior choroidal fissure, between the crus of fornix and the pulvinar (Fig. 6). Three hemispheres (13%) presented this pattern in our study. Pattern B can also be subdivided into 2 groups: B1 (single trunk, 1 hemisphere; 4%) and B2 (2 or more trunks, 2 hemispheres; 9%).
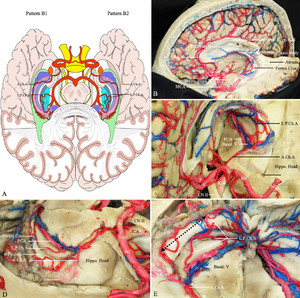
Pattern B of the LPChA: anatomical and artistic illustrations.A:Illustration of the subdivision of pattern B. The left side shows pattern B1, which presents as a single trunk entering the posterior choroidal fissure above the crus of fornix. The right side shows pattern B2 of the LPChA, which presents as 2 or more trunks of the LPChA. Artist: Yuanzhi Xu.B:The left parietal, occipital, and temporal lobes have been removed to reveal the LPChA trajectory.C:Enlargement of thedashed boxlabeled in panel B. The LPChA presents as a single trunk (pattern B1) that enters the posterior choroidal fissure between the crus of fornix and the pulvinar.D和E:Superior (D) and medial (E) views of the right hippocampus in the same specimen. The LPChA presents as double trunks that enter the posterior choroidal fissure between the crus of fornix and the pulvinar (pattern B2). In this situation, the distance between the AChA and LPChA (dotted line) is very large and the LPChA will not be encountered in anterolateral and lateral approaches. A. = artery; ACA = anterior cerebral artery; A.Ch.A. = anterior choroidal artery; CN = cranial nerve; Corp. Call. = corpus callosum; Hippo. = hippocampal; Lat. = lateral; L.P.Ch.A. = lateral posterior choroidal artery; MCA = middle cerebral artery; Plex. = plexus; V. = vein; Vent. = ventricle. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Pattern C
This pattern is also called the “mixed pattern” because it presented features of both patterns A and B. Two hemispheres (9%) presented this pattern.
Microsurgical Approaches to the LPChA
Four surgical approaches—transsylvian trans–limen insulae, lateral transtemporal, transparietal transcortical, and contralateral posterior interhemispheric transfalcine transprecuneus—were performed consecutively in all hemispheres to investigate anterolateral, lateral, and posterolateral views and key landmarks for the LPChA (Figs. 7–9,Table 2).
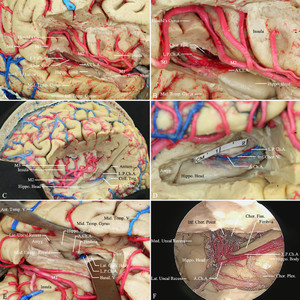
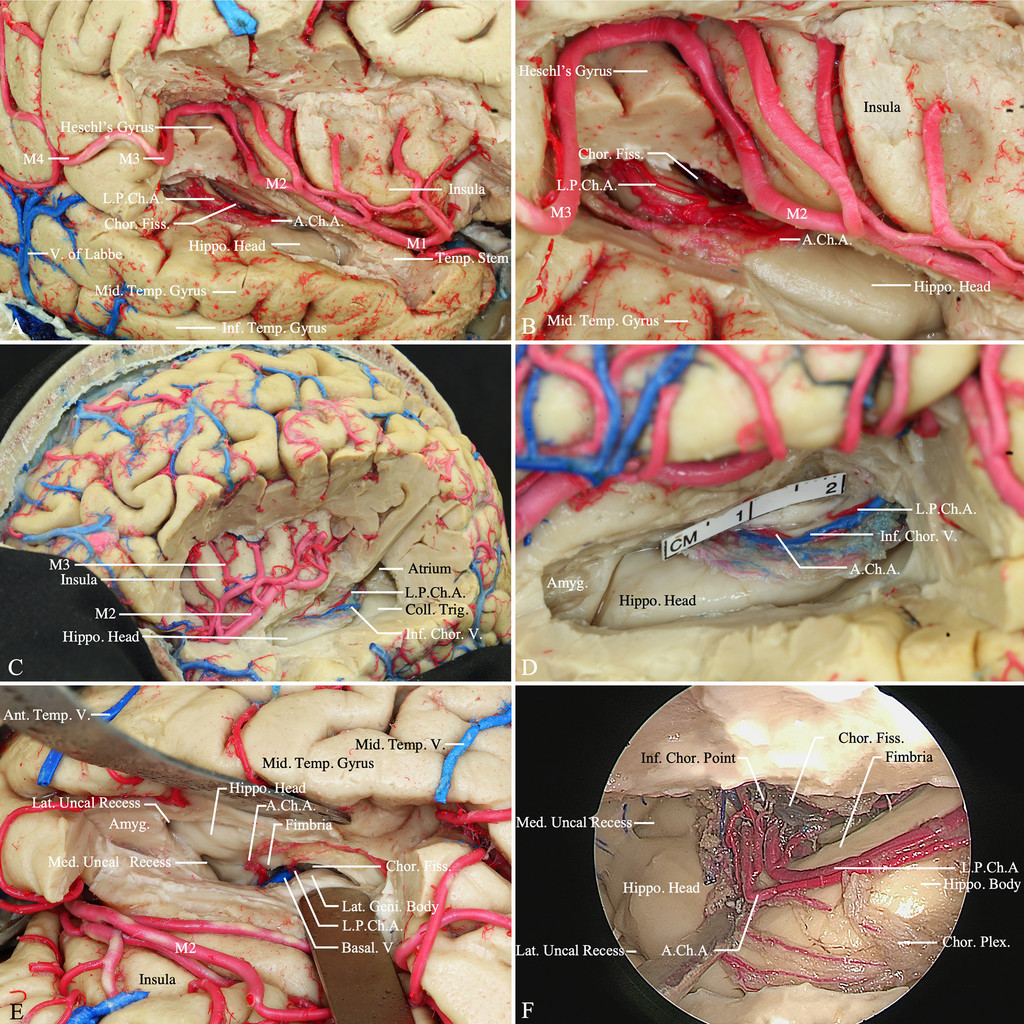
Transsylvian trans–limen insulae approach to the LPChA.A:Transsylvian trans–limen insulae approach, right hemisphere—the frontal and parietal opercula have been removed to facilitate studying the LPChA from this trajectory; the sylvian fissure is opened widely, and the inferior insular sulcus is used to access the temporal horn and hippocampal head. The choroid plexus is identified immediately posterior to the hippocampal head.B:Enlarged view of panel A. The forniceal segment of the LPChA can be identified entering the choroidal fissure posterior to the inferior choroidal point to run along the superior surface of the fimbria and by the medial part of the choroid plexus.C:Transsylvian trans–limen insulae approach, left hemisphere—the frontal, temporal, and parietal opercula have been removed.D:Enlarged view of panel C. The LPChA can be observed entering the choroidal fissure approximately 8 mm posterior to the inferior choroidal point, AChA, and inferior choroidal vein.E:Transsylvian trans–limen insulae approach in a different specimen; the opercula have been preserved. The LPChA enters the anterior choroidal fissure, between the fimbria and LGB and posterior to AChA.F:Endoscopy-assisted transsylvian trans–limen insulae approach in another specimen. Note the close distance between the AChA and LPChA at the inferior choroidal point. A. = artery; A.Ch.A. = anterior choroidal artery; Amyg. = amygdala; Ant. = anterior; Chor. = choroid, choroidal; Coll. Trig. = collateral trigone; Fiss. = fissure; Hippo. = hippocampus; Inf. = inferior; Lat. = lateral; Lat. Geni. Body = lateral geniculate body; L.P.Ch.A. = lateral posterior choroidal artery; Med. = medial; Mid. = middle; Temp. = temporal; V. = vein. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Lateral transtemporal and transparietal transcortical approaches to the LPChA.A:Lateral transtemporal approach—a right frontotemporal craniotomy has been completed to expose the temporal lobe. A corticectomy is made along the middle temporal gyrus, usually starting 2 cm posterior to the temporal pole and extending posteriorly for 3–4 cm (dashed line) to enter the temporal horn.B:The choroid plexus, hippocampal head, and hippocampal body are easily identified in this approach. The choroid plexus is elevated to expose the choroidal fissure, and 2 trunks of LPChA are encountered in this specimen.C:Right lateral transtemporal approach in a different specimen; a single LPChA trunk is identified entering the anterior choroidal fissure (pattern A1).D:Left transparietal transcortical approach—the atrium of the lateral ventricle has been accessed by a cortical incision through the superior parietal lobe. The pulvinar, crus of fornix, and posterior choroidal fissure between them are identified. The LPChA runs between the pulvinar and the crus of fornix and provides terminal branches to the pulvinar.E:The right transparietal approach reveals the pulvinar segment of the LPChA, which starts at the posterior choroidal fissure and terminates in the pulvinar.F:Endoscopy-assisted view in the same specimen as E. The calcar avis and bulb of corpus callosum serve as landmarks on the medial wall of the atrium; the collateral trigone forms the floor of the atrium. The LPChA runs between the pulvinar and the crus of fornix, which serve as the anterior wall of the atrium. A.Ch.A. = anterior choroidal artery; Ant. = anterior; Cer. = cerebral; Chor. = choroid, choroidal; Coll. Trig. = collateral trigone; Corp. Call. = corpus callosum; Fiss. = fissure; Front. = frontal; Hippo. = hippocampus; Inf. = inferior; Intrapar. = intraparietal; Lat. Geni. Body = lateral geniculate body; L.P.Ch.A. = lateral posterior choroidal artery; Mid. = middle; Par. = parietal; Plex. = plexus; Post. = posterior; Subpar. = subparietal; Sulc. = sulcus; Sup. = superior; Syl. = sylvian; Temp. = temporal; Unc. = uncal; V. = vein; Vent. = ventricle. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Contralateral posterior interhemispheric transfalcine transprecuneus approach to the LPChA.A:Contralateral posterior interhemispheric transfalcine transprecuneus approach (arrow) is illustrated in a dissected left hemisphere in which the frontal lobe, parietal lobe, and thalamus have been removed. This approach is designed to run from the contralateral posterior interhemisphere to the ipsilateral precuneus and trigonal lesions, and it provides a wider operative corridor with avoidance of optic radiations’ interruption.B:Medial surface of the left hemisphere. The precuneus is located between the parieto-occipital sulcus, ascending ramus of the cingulate sulcus, and subparietal sulcus (light-green shadow).C:Enlargement of panel A in ventricle region shows LPChA running medially along the choroid plexus, and the contralateral transprecuneus approach provides direct access to the pulvinar segment of the LPChA and to the posterior forniceal segment.D:A step-by-step microsurgical dissection of contralateral posterior interhemispheric transfalcine transprecuneus approaches. The craniotomy is completed on the contralateral superior parietal lobule region, and then the dura mater is incised in a horseshoe-shaped fashion based on the superior sagittal sinus, in which the falx, contralateral parietal occipital sulcus, precuneus, and cuneus are exposed.E:The falx between the superior and inferior sagittal sinus is resected to provide access to the ipsilateral precuneus over the atrium.F:A cortical incision through the precuneus is performed, and the superior and medial wall of the atrium is cut. The choroid plexus and LPChA are revealed.G:Endoscopy-assisted view in the same specimen as shown in panel F. The posterior forniceal and pulvinar segment of LPChA runs above the prominent C-shaped hippocampus in the medial border of the choroid plexus, and then in the level of the choroidal glomus it curves anteriorly and is involved in the crus of fornix and the pulvinar. A. = artery; A.Ch.A. = anterior choroidal artery; Ant. = anterior; Asc. = ascending; Call. = callosum; Cer. = cerebral; Chor. = choroid, choroidal; Cing. = cingulate; CN = cranial nerve; Comm. = commissure; Corp. Call = corpus callosum; Gr. = greater; Hippo. = hippocampus; Inf. = inferior; Inforb. = infraorbital; Int. = interior; Lac. = lacrimal; L.P.Ch.A. = lateral posterior choroidal artery; Max. = maxillary; M.P.Ch.A. = medial posterior choroidal artery; N. = nerve; Occip. = occipital; Palat. = palatine; Par. = parietal; Paracent. = paracentral; Peri. = pericallosal; Post. = posterior; Sag. = sagittal; Str. = straight; Subpar. = subparietal; Sulc. = sulcus; Sup. = superior; V. = vein. Copyright Juan Carlos Fernandez-Miranda. Published with permission. Figure is available in color online only.
Surgical approaches to the LPChA
| Approach | Segmental View | Key Landmarks | Pattern of LPChA |
|---|---|---|---|
| Transsylvian trans–limen insulae | Cisternal + forniceal (anterior) | Amygdala, choroid plexus, hippocampal head, inferior choroidal point, AChA, basal vein, PCA, oculomotor nerve | A |
| Lateral transtemporal | 池状的(后)+ forniceal | Choroid plexus, collateral eminence, hippocampal head & body, inferior choroidal point, AChA, basal vein, PCA | C |
| Transparietal transcortical/superior parietal lobule | Forniceal (posterior) + pulvinar | Choroid plexus, crus of fornix, pulvinar, collateral trigone, calcar avis, bulb of corpus callosum | B |
| Contralateral posterior interhemispheric transfalcine transprecuneus | Forniceal (posterior) + pulvinar | Precuneus, choroid plexus, crus of fornix, pulvinar, collateral trigone | B |
In the transsylvian trans–limen insulae approach, after wide splitting of thesylvian fissure, the uncus,limen insulae, and inferior limiting sulcus were exposed; removal of theamygdala, which is located within the anterior half of the uncus and forms the anterior wall of the temporal horn, provides access to the ventricle and exposure of thehippocampal head.10Further expansion of this corridor requires extending the corticectomy to the limen insulae and anterior-most aspect of theinferior limiting sulcus of the insula. The choroid plexus is identified immediately posterior to the hippocampal head, and its retraction toward the roof of the temporal horn facilitates recognition of the inferior choroidal point, anterior choroidal fissure, and the entrance of AChA and exit of the inferior ventricular vein. The choroidal segment of the LPChA can often be identified entering the choroidal fissure at an average of 8 mm posterior to the inferior choroidal point (pattern A) to run along the superior surface of the fimbria and by the medial part of the choroid plexus. In cases of posterior entrance into the choroidal fissure (pattern B), the forniceal segment of the LPChA will not be accessible (Fig. 7).
To expose the cisternal segment of the LPChA, first the choroidal fissure is opened proximal to the LPChA entrance and all the way anterior to reach the inferior choroidal point. Next, the basal vein and PCA (P2P segment) are exposed within the ambient cistern and the LPChA origin from the PCA is identified. Last, for full exposure of the cisternal segment of the LPChA and its trunks, an incision is made along the medial aspect of the uncal recess from the inferior choroidal point to the uncal apex by working inside the ventricle just above the hippocampal head. This medial disconnection of the hippocampal head provides exposure from the ambient to the oculomotor and opticocarotid cisterns.
In the lateral transtemporal approach, once thetemporal lobeis exposed, a corticectomy is made along the middle temporal gyrus, usually starting 2 cm posterior to the temporal pole and extending posteriorly for 3–4 cm (5 cm posterior to the temporal pole on the dominant hemisphere and 6 cm on the nondominant hemisphere).11另外,临时低劣oral sulcus can be used for a transsulcal approach. After the temporal horn is entered, the choroid plexus, collateral eminence, and hippocampal head and body are identified. The choroid plexus is elevated to expose and open the choroidal fissure. In comparison with the transsylvian approach, the lateral transtemporal provides a more direct approach to the forniceal segment of the LPChA, including for those cases with posterior entrance (pattern B), but does not allow access to the anterior aspect of the cisternal segment (Fig. 8A–C).
In the transparietal transcortical approach, the atrium of the lateral ventricle is accessed by a cortical incision through thesuperior parietal lobuleor via theintraparietal sulcus.12Once the choroid plexus is identified, its retraction anteriorly and medially exposes the pulvinar and crus of fornix and the posterior choroidal fissure between them. The calcar avis and bulb of thecorpus callosumserve as landmarks on the medial wall of the atrium, and the collateral trigone forms the floor. The LPChA runs between the pulvinar and crus of fornix and provides terminal branches to the pulvinar. Of note, if there is an inferior LPChA trunk running in the fimbrio-dentate sulcus or parahippocampus gyrus, it crosses the fornix and stops at the ventricular surface of the pulvinar (Fig. 8D–F).
In the contralateral posterior interhemispheric transfalcine transprecuneus approach, the superior and medial wall of the contralateral atrium is incised through theprecuneus, which is located between theascending ramus of the cingulate sulcus, the parieto-occipital sulcus, and the subparietal sulcus (Fig. 9A–C).13When the atrium is exposed, several surgical landmarks, such as the choroid plexus, pulvinar, hippocampus, and crus of fornix, can be distinguished. The posterior forniceal and pulvinar segments of the LPChA run above the prominent C-shaped hippocampal tail at the medial border of the choroid plexus, and then at the level of the choroidal glomus the LPChA curves anteriorly to travel between the crus of fornix and the pulvinar. The inferior LPChA trunk usually runs in the ambient and quadrigeminal cisterns, and its identification requires opening the choroidal fissure between the fornix and the pulvinar (Fig. 9D–F).
In comparison with the previous 2 approaches (transsylvian trans–limen insulae and lateral transtemporal), the transparietal and contralateral transprecuneus approaches provide direct access to the pulvinar segment of the LPChA and to the posterior forniceal segment, including for those cases with posterior choroidal entrance (pattern B). However, it does not allow access to the cisternal segment or the anterior aspect of the forniceal segment in transparietal and contralateral transprecuneus approaches.
Case Illustration
Peri-Atrial Meningioma
VIDEO 1.Contralateral posterior interhemispheric transfalcine transprecuneus approach performed in a peri-atrial meningioma case. Copyright Aaron Cohen-Gadol. Published with permission from The Neurosurgical Atlas by Aaron Cohen-Gadol. Clickhereto view.
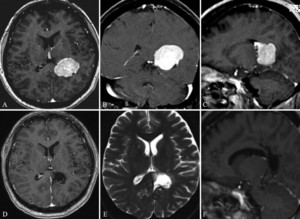
Peri-atrial meningioma.A–C:Preoperative contrast-enhanced MR images show a tumor with relatively homogeneous enhancement and a dural tail along the choroid plexus in the left trigone area of the lateral ventricle.D–F:The postoperative MR images show gross-total resection. Copyright Aaron Cohen-Gadol. Published with permission fromThe Neurosurgical Atlasby Aaron Cohen-Gadol.
The patient had a remarkable improvement at 3 weeks’ follow-up, and postoperative MRI showed a gross-total resection (Fig. 10D–F).
讨论
Here we have investigated the detailed microsurgical anatomy of the LPChA and its surgical implications. Most frequently, 2 LPChAs were noticed in our study, which is in accordance with the observations of previous investigators.9However, some other studies have declared up to 9 possible LPChAs.14这种差异的原因可能是相关的to the number of specimens studied. However, we speculate that other studies classified as LPChAs several small plexal branches originating from the PCA that actually terminated in the dentate gyrus and served as posterior hippocampal–parahippocampal arteries. In our study, we applied clear criteria to identify LPChA as an artery running along the choroid plexus to terminate at the posterior aspect of the choroid plexus and the pulvinar.
In our study, the LPChA arose from the main PCA trunk in most specimens distal (and lateral) to the medial posterior choroidal artery (MPChA). In a minority of cases, it can arise from other PCA branches, such as the calcarine, anterior temporal, posterior temporal, or splenial artery, as shown in our study and others.5,6,8An important contribution of our study is the introduction of the “pulvinar segment” or terminal segment of the LPChA. The pulvinar is divided into a lateral superior ventricular surface and a medial inferior cisternal surface by the crus of fornix and the choroidal fissure. When there are double trunks, the superior trunk runs along the ventricular surface of the pulvinar, whereas the inferior trunk runs along the cisternal surface of the pulvinar.
无意的手术或栓子阻塞的LPChA may cause 3 neurological manifestations: visual field defect, sensorimotor dysfunction, and cognitive deficits (e.g., aphasia, memory disturbances). This is consistent with our study, which showed terminal branches to the parahippocampus, hippocampus, LGBs, choroid plexus, and pulvinar. However, the severity of neurological sequelae after LPChA injury was quite variable in a previous study.14这可以解释的存在丰富的轶事tomoses between the LPChA and AChA within the choroid plexus,6and by the frequent existence (70%) of multiple LPChA trunks, as demonstrated in this study.
LPChA应该主要考虑手术in the microsurgical management of lateral ventricular tumors because it may be encased or attached to the tumor surface, and it may provide direct vascular supply to the lesion. Saito and colleagues revealed that in their study, 30% of patients had infarction in the peri-atrial/periventricular regions after coagulation of the choroid plexus at the atrium, corresponding to the territory of the LPChA.15Surgical manipulation of the choroid plexus in order to achieve hemostasis is inevitable, but according to our study, 5 surgical pearls and pitfalls can be considered: 1) the LPChA trunk typically runs in the medial border of the choroid plexus, which may facilitate its recognition during surgery; 2) the distance between the AChA at the inferior choroidal point and the LPChA is a valuable reference during surgery, but there are cases of posterior choroidal entrance; 3) most frequently there are 2 or more LPChA trunks, which makes possible the sacrifice of one trunk feeding the tumor while preserving the other that provides supply to relevant structures; 4) coagulation of the LPChA should be performed at the forniceal segment rather than at the cisternal segment, where branches to the thalamus are more frequent; and 5) intraventricular approaches can be selected based on the tumor location and the LPChA anatomy (lateral transtemporal approaches provide a wider surgical field to access the forniceal segment of the LPChA regardless of its choroidal entrance, transsylvian approaches offer excellent access to the cisternal segment and anterior choroidal entrance, and transparietal and contralateral posterior interhemispheric transfalcine transprecuneus approaches are better suited for lesions involving the atrium and terminal segment of the LPChA). Therefore, careful surgical technique when opening the choroidal fissure to distinguish the location of the LPChA and prudent coagulation in the medial aspect of the choroid plexus are necessary.
Conclusions
The LPChA runs along the choroidal fissure medial to the AChA and supplies the pulvinar region. The microanatomical features of the LPChA are of great neurosurgical significance when performing surgery for lateral ventricular lesions. Meticulous protection of this vessel during surgery is crucial for successful outcomes.
致谢
Dr. Xu was supported by Young Faculty’s Research Ability Training Overseas of the Development Project of High Level University in Shanghai as a visiting scholar.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Author Contributions
Conception and design: Xu. Acquisition of data: Xu, Mohyeldin, Doniz-Gonzalez, Vigo, Pastor-Escartin, Meng, Cohen-Gadol. Analysis and interpretation of data: Xu. Drafting the article: Xu. Critically revising the article: Fernandez-Miranda, Xu, Cohen-Gadol. Reviewed submitted version of manuscript: Fernandez-Miranda, Xu. Approved the final version of the manuscript on behalf of all authors: Fernandez-Miranda. Statistical analysis: Fernandez-Miranda. Administrative/technical/material support: Fernandez-Miranda. Study supervision: Fernandez-Miranda.
Supplemental Information
Videos
Video 1.https://vimeo.com/469736778.
References
-
1 ↑
BeevorCE.On the distribution of the different arteries supplying the human brain.Proc R Soc Lond B Biol Sci.1909;200:1–55.
-
3 ↑
HudsonAJ.The development of the vascular pattern of the choroid plexus of the lateral ventricles.J Comp Neurol.1960;115:171–186.
-
4 ↑
GallowayJR,GreitzT.The medial and lateral choroid arteries. An anatomic and roentgenographic study.Acta Radiol.1960;53:353–366.
-
5 ↑
FujiiK,LenkeyC,RhotonALJr.Microsurgical anatomy of the choroidal arteries: lateral and third ventricles.J Neurosurg.1980;52(2):165–188.
-
6 ↑
MarinkovićS,GiboH,MilisavljevićM,et al.Microanatomy of the intrachoroidal vasculature of the lateral ventricle.开云体育app官方网站下载入口.2005;57(1)(suppl):22–36.
-
7
NagataS,RhotonALJr,BarryM.Microsurgical anatomy of the choroidal fissure.Surg Neurol.1988;30(1):3–59.
-
8 ↑
VinasFC,LopezF,DujovnyM.Microsurgical anatomy of the posterior choroidal arteries.Neurol Res.1995;17(5):334–344.
-
9 ↑
Wolfram-GabelR,MaillotC,KoritkéJG,LaudeM.The vascularization of the human tela choroidea of the lateral ventricle. Article in French.Acta Anat (Basel).1987;128(4):301–321.
-
10 ↑
Fernandez-MirandaJC,de OliveiraE,RubinoPA,et al.Microvascular anatomy of the medial temporal region: part 1: its application to arteriovenous malformation surgery.开云体育app官方网站下载入口.2010;67(3 Suppl Operative):ons237–ons276.
-
11 ↑
WheatleyBM.Selective amygdalohippocampectomy: the trans-middle temporal gyrus approach.Neurosurg Focus.2008;25(3):E4.
-
12 ↑
CiklaU,SwansonKI,TumturkA,et al.Microsurgical resection of tumors of the lateral and third ventricles: operative corridors for difficult-to-reach lesions.J Neurooncol.2016;130(2):331–340.
-
13 ↑
BohnstedtBN,KulwinCG,ShahMV,Cohen-GadolAA.Posterior interhemispheric transfalcine transprecuneus approach for microsurgical resection of periatrial lesions: indications, technique, and outcomes.J Neurosurg.2015;123(4):1045–1054.
-
14 ↑
ZealAA,RhotonALJr.Microsurgical anatomy of the posterior cerebral artery.J Neurosurg.1978;48(4):534–559.
-
15 ↑
SaitoR,KumabeT,SonodaY,et al.Infarction of the lateral posterior choroidal artery territory after manipulation of the choroid plexus at the atrium: causal association with subependymal artery injury.J Neurosurg.2013;119(1):158–163.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}