
Publicationof the Management of Myelomeningocele Study (MOMS) ushered in a new paradigm for the early management of children with myelomeningocele. The MOMS trial showed that open fetal surgery for myelomeningocele reduced the chance of a child requiring a shunt for hydrocephalus and came with acceptable risks for the mother and fetus.1Subsequent studies have shown that patients having fetal surgery are more likely to ambulate early in life, have equal early cognitive outcomes, and have an improved quality of life compared with children treated with postnatal surgery.2–4
An increasing body of literature has suggested that race and ethnicity and social determinants of health such as income, wealth, insurance status, and education level can have a profound effect on health outcomes, quality of life, and mortality.5–7A previous study showed that sociodemographic factors had a significant influence on continence and ambulatory status in a large cohort of patients with spina bifida.8Identifying preventable health disparities is critical to improving the outcomes and quality of life for patients with chronic diseases such as spina bifida. We sought to determine the sociodemographic background of patients who underwent fetal surgery for spina bifida compared with those who underwent traditional postnatal surgery.
开云体育世界杯赔率
Data Collection
Since 2009, patients receiving care through the Multidisciplinary Spina Bifida Clinic at Children’s Wisconsin have been included in the National Spina Bifida Patient Registry (NSBPR). The NSBPR is a typical disease-based patient registry, partially funded and managed by the Centers for Disease Control and Prevention. There are 24 clinics across the country that participate in data entry for the registry. Data are collected on a yearly basis through interviews and examinations by the multidisciplinary treatment team. The NSBPR variables are recorded and then abstracted and entered anonymously into the database system. Each participating clinic has access to its own population data.
2019年9月,对儿童NSBPR数据库’s Wisconsin was queried for children with myelomeningocele born in the United States and its territories between 2000 and 2019. The Children’s Wisconsin IRB approved this study. The following variables were abstracted: year of birth, sex, the method of myelomeningocele repair, primary and secondary insurance at the time of the query, residential zip code at the time of the query, and race and ethnicity. The zip code was used to determine the median household income for individual zip code tabulation areas using the US Census Bureau 2013–2017 American Community Survey 5-year estimates in February 2020 (https://data.census.gov/cedsci/). In February 2020, zip code was also used to determine the 2018 Distressed Communities Index (DCI) score, a composite socioeconomic ranking with scores ranging from 0 (no distress) to 100 (severe distress).9The DCI is a product of the Economic Innovation Group, a bipartisan public policy organization. The DCI for each residential zip code is based on the following 7 components: level of education in the adult population, housing vacancy rate, unemployment, poverty rate, median income ratio, change in employment, and change in number of business establishments. This is an established metric increasingly used to determine the effect of community distress on medical risks and outcomes.10,11
Statistical Analysis
Statistical analysis was performed using R version 3.6.2 (The R Project). For categorical variables, each category and its frequency were computed, 95% confidence intervals were calculated, and the chi-square test was used to examine the relationship between the categorical variables for the postnatal and fetal surgery groups. Continuous variables were analyzed using mean and standard deviation within each group and compared between groups using the t-test. The significance level was set at p = 0.05.
Results
Overall, 205 patients were identified, 23 who had undergone fetal surgery and 182 who had undergone postnatal surgery (Table 1). Sixteen patients were "entered not enrolled" in the registry. These patients are treated at our center, but their families have not consented to enrollment and data collection for the NSBPR and, therefore, they are not part of the 205 patients in this study. There was a significant difference in the mean age of the two groups at the time of data collection (9.99 years postnatal surgery vs 6.0 years fetal surgery, p = 0.002), likely due to the increased availability of fetal surgery following publication of the MOMS in 2011. Only 3 of the patients who underwent fetal surgery were born between 2000 and 2010. There was a similar sex distribution between the fetal surgery and postnatal surgery groups (female 47.8% vs 53.8%, p = 0.746).
Patient demographics and characteristics
| Characteristic | 胎儿手术(n = 23) | Postnatal Surgery (n = 182) | p Value |
|---|---|---|---|
| Sex, n (%) [95% CI] | 0.746 | ||
| F | 11 (47.8) [26.8–69.4] | 98 (53.8) [46.3–61.2] | |
| M | 12 (52.2) [30.6–73.2] | 84 (46.2) [38.8–53.7] | |
| Mean age, yrs (SD)* | 6.00 (5.28) | 9.99 (5.15) | 0.002 |
| Race & ethnicity, n (%) [95% CI] | 0.058 | ||
| Hispanic | 1 (4.3) [0.1–21.9] | 28 (15.4) [10.5–21.5] | |
| Non-Hispanic African American | 0 (0.0) [0–14.8] | 22 (12.1) [7.7–17.7] | |
| Non-Hispanic White | 22 (95.7) [78.1–99.9] | 125 (68.7) [61.4–75.3] | |
| Other | 0 (0.0) [0–14.8] | 7 (3.8) [1.6–7.8] | |
| Primary insurance, n (%) [95% CI] | <0.001 | ||
| 商业 | 23 (100.0) [85.2–100] | 95 (52.2) [44.7–59.6] | |
| Medicaid | 0 (0.0) [0–14.8] | 80 (44.0) [36.6–51.5] | |
| Other | 0 (0.0) [0–14.8] | 7 (3.8) [1.6–7.8] | |
| Unknown | 0 | 0 | |
| DCI score | 0.289 | ||
| Mean (SD) | 31.27 (29.87) | 38.46 (30.76) | |
| Unknown, n | 0 | 11 | |
| Median household income by residential zip code | 0.122 | ||
| Mean (SD) | $66,507.35 ($21,123.30) | $59,133.01 ($17,762.90) | |
| Unknown, n | 0 | 12 |
Age at the time of data collection.
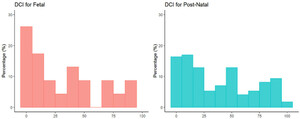
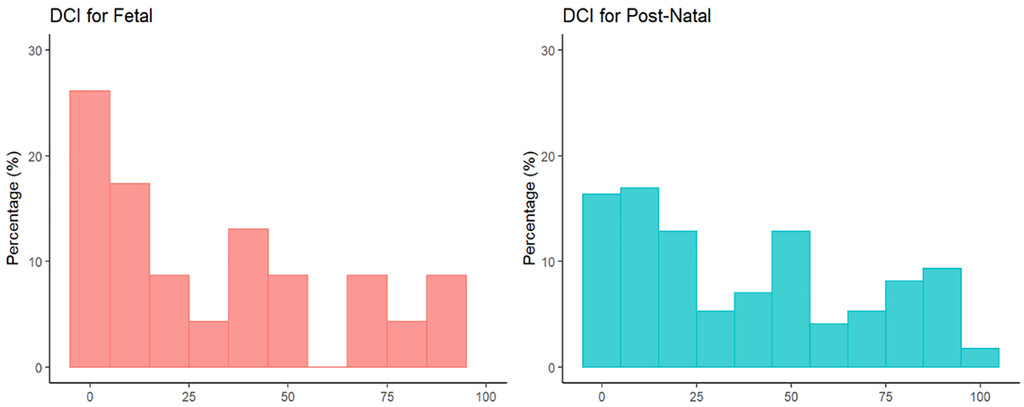
There was a significant difference in insurance status between the two groups, with 100% of the fetal surgery group and only 52.2% of the postnatal group having primary commercial insurance (p < 0.001). The overall hospital commercial insurance rate in 2019 was 52% (personal communication, hospital leadership). Patients who had undergone fetal surgery were also more likely to have a non-Hispanic White racial and ethnic background; however, this just missed the level of statistical significance (95.7% vs 68.7%, p = 0.058). The median household income based on the residential zip code showed that patients who had undergone fetal surgery tended to reside in areas with greater income (mean $66,507 vs $59,133, p = 0.122) and also tended to reside in areas with less community distress (mean DCI score 31.3 vs 38.5, p = 0.289); however, these differences did not reach the level of statistical significance. The highest quartile of DCI scores (> 75) is represented by communities that are severely distressed. In the fetal surgery group, 13.0% of patients came from communities considered significantly distressed, whereas 19.3% of patients in the postnatal surgery group came from significantly distressed communities (Fig. 1). Of note, only 2 patients who had undergone postnatal surgery had a change in residential zip code over time in the NSBPR, both due to military service. All other residential zip codes were unchanged over time.

Bar graphs showing the distribution of DCI scores for the fetal surgery (left) and postnatal surgery (right) groups, where 0 is minimally distressed and 100 is severely distressed. There was a general trend toward patients in the fetal surgery group residing in less-distressed communities. Figure is available in color online only.
Discussion
This retrospective review of patients treated at a single, multidisciplinary spina bifida clinic showed a statistically significant difference in insurance status in patients who were treated with fetal surgery compared with those who were treated with postnatal surgery. All patients in the fetal surgery group had primary commercial insurance compared with only 52.2% of the postnatal surgery group. In addition, nearly all patients in the fetal surgery group had a non-Hispanic White racial and ethnic background compared with 68.7% of the postnatal surgery group, although this difference fell short of statistical significance. Patients who had undergone fetal surgery tended to live in less-distressed communities and communities with higher household income, yet these findings did not rise to the level of statistical significance. While our data are limited by a small sample size, the sociodemographic disparities noted in this preliminary study suggest that further study is warranted.
Publication of the MOMS trial in 2011 marked a turning point in the care of children with myelomeningocele.1This cohort of patients has been the subject of longitudinal studies over the last several years. Many of the improvements noted in the prenatal surgery group have been sustained as the children have become school aged.2,3
虽然妈妈通知的患者群uch of our knowledge about open fetal surgery for myelomeningocele, little attention has been paid to the sociodemographic characteristics of the study population. In the MOMS, 94% of the mothers in the prenatal surgery group and 92% of the mothers in the postnatal surgery group were White. Greater than 90% of the trial population mothers were married or living with their partner. The average lengths of maternal schooling were 14.8 years and 15.0 years in the prenatal and postnatal surgery groups, respectively.1Insurance status was not reported. These data suggest a study population with a high degree of social stability that is racially and ethnically homogeneous and well educated. Similar sociodemographic characteristics are found in post-MOMS fetal surgery cohorts reported in the literature.12,13
In comparison, a review of more than 2000 patients enrolled in the NSBPR gives a sense of the typical sociodemographic characteristics of the population of myelomeningocele patients. This review showed that 64.5% of patients had a non-Hispanic White racial and ethnic background and only 44.7% of patients had primary commercial insurance.14Further study of this patient population showed that factors such as insurance status and race and ethnicity played a role in determining health outcomes.8
现在仍不知道是否患者脊柱bifida from a more diverse sociodemographic background treated with fetal surgery would have the same sustained improvements as those observed in the MOMS cohort. While the number of fetal surgery centers dramatically increased after the publication of the MOMS results, the intervention still requires a significant investment of time and effort on the part of the mother and family. Many families must travel far from home to a fetal center for the workup, surgery, and postsurgical care. Following surgery, the patient will spend several nights in the hospital and 2 weeks on modified bedrest and have weekly follow-up at most fetal surgery centers.1,15This is a significant commitment, often taking families away from income-producing labor and social support for weeks or months. Families must also factor in the expenses that will be incurred once the child is born. The first few years of life are frequently a financially challenging time for families of children with spina bifida.16
Pediatric neurosurgeons continue to enjoy a prominent role in our society, and this gives us the unique ability to advocate for our patients.17在地方和区域层面,cente胎儿手术rs would be wise to have resources available for families with economic instability and less-robust social support. Outreach to community primary care physicians and obstetricians may help to limit disparities in the provision of care for mothers who are pregnant with a child with spina bifida. While fetal surgery is an expensive procedure with great costs to the healthcare system, the potential long-term improvement in outcomes for patients treated with fetal surgery may make the early investment worthwhile.18
There are a number of limitations to this study. As a single-center study, the number of patients, particularly in the fetal surgery cohort, is small. This limits the power of our conclusions. While there was a trend toward patients in the fetal surgery cohort residing in zip codes with higher median income and less community distress, these data did not rise to the level of statistical significance given the small sample size. Furthermore, all these metrics are imperfect markers of socioeconomic well-being. The NSBPR does not collect data on the level of parent education, parental occupation, or whether the parents of the child live together. Furthermore, while a large percentage of families in our spina bifida clinic choose to participate in the NSBPR, the registry does not represent all children with spina bifida treated at our center. At our most recent analysis of the institutional NSBPR data, 16 patients were not captured in the registry and not included in our study. Finally, between 2000 and 2010, the access to fetal surgery for patients was limited by the MOMS trial, which required travel to one of three centers and randomization to postnatal surgery for some of the patients included in the MOMS.
Conclusions
Our limited single-center data suggest that sociodemographic and racial and ethnic disparities exist regarding access to fetal surgery for myelomeningocele. Further study of the complete NSBPR is warranted, and efforts to mitigate healthcare disparities in this patient population should be pursued.
Acknowledgments
The National Spina Bifida Patient Registry is funded by the National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention, Atlanta, Georgia. Preparation of this manuscript was supported by grant no. 6 U01DD001240-01-01.
We would like to thank Anika Szabo, PhD, and Bi Qing Teng for their assistance with statistical analysis.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Author Contributions
Conception and design: Foy. Acquisition of data: Foy, Derflinger, Sherburne. Analysis and interpretation of data: Foy, Sawin, Heffelfinger, Koop, Cohen, Sherburne. Drafting the article: Foy, Sherburne. Critically revising the article: Foy, Sawin, Heffelfinger, Koop, Cohen, Sherburne. Reviewed submitted version of manuscript: Foy. Approved the final version of the manuscript on behalf of all authors: Foy. Study supervision: Foy.
Supplemental Information
Previous Presentations
This work was presented at the 49th Annual Meeting of the AANS/CNS Section on Pediatric Neurological Surgery, December 2–4, 2020, held virtually.
References
-
1 ↑
AdzickNS,ThomEA,SpongCY,BrockJW III,BurrowsPK,JohnsonMP,et al.A randomized trial of prenatal versus postnatal repair of myelomeningocele.N Engl J Med.2011;364(11):993–1004.
-
2 ↑
FarmerDL,ThomEA,BrockJW III,BurrowsPK,JohnsonMP,HowellLJ,et al.The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes.Am J Obstet Gynecol.2018;218(2):256.e1–256.e13.
-
3 ↑
HoutrowAJ,ThomEA,FletcherJM,BurrowsPK,AdzickNS,ThomasNH,et al.Prenatal repair of myelomeningocele and school-age functional outcomes.Pediatrics.2020;145(2):e20191544.
-
4 ↑
MummareddyN,DewanMC,HuangA,et al.Intrauterine closure of myelomeningocele is associated with superior long-term quality of life than postnatal closure: a single-center study.J Neurosurg Pediatr.2019;24(2):115–119.
-
5 ↑
GaleaS,TracyM,HoggattKJ,DimaggioC,KarpatiA.Estimated deaths attributable to social factors in the United States.Am J Public Health.2011;101(8):1456–1465.
-
6
KulkarniAV,CochraneDD,McNeelyPD,ShamsI.Medical, social, and economic factors associated with health-related quality of life in Canadian children with hydrocephalus.J Pediatr.2008;153(5):689–695.
-
7 ↑
SekeresMA.Children’s Health, Nation’s Wealth: Assessing & Improving Child Health.National Academies Press;2004.
-
8 ↑
SchechterMS,LiuT,SoeM,SwansonM,WardE,ThibadeauJ.Sociodemographic attributes and spina bifida outcomes.Pediatrics.2015;135(4):e957–e964.
-
9 ↑
Distressed Communities Index. Economic Innovation Group.Accessed October 28, 2021.https://eig.org/dci/2018-dci-map-national-zip-code-map
-
10 ↑
TracyBM,SmithRN,MillerK,ClaytonE,BaileyK,GerrinC,et al.Community distress predicts youth gun violence.J Pediatr Surg.2019;54(11):2375–2381.
-
11 ↑
MehaffeyJH,HawkinsRB,CharlesEJ,TurrentineFE,HallowellPT,FrielC,et al.Socioeconomic "Distressed Communities Index" improves surgical risk-adjustment.Ann Surg.2020;271(3):470–474.
-
12 ↑
BennettKA,CarrollMA,ShannonCN,BraunSA,DabrowiakME,CrumAK,et al.Reducing perinatal complications and preterm delivery for patients undergoing in utero closure of fetal myelomeningocele: further modifications to the multidisciplinary surgical technique.J Neurosurg Pediatr.2014;14(1):108–114.
-
13 ↑
MoldenhauerJS,SoniS,RintoulNE,SpinnerSS,KhalekN,Martinez-PoyerJ,et al.Fetal myelomeningocele repair: the post-MOMS experience at the Children’s Hospital of Philadelphia.Fetal Diagn Ther.2015;37(3):235–240.
-
14 ↑
SawinKJ,LiuT,WardE,ThibadeauJ,SchechterMS,SoeMM,WalkerW.The National Spina Bifida Patient Registry: profile of a large cohort of participants from the first 10 clinics.J Pediatr.2015;166(2):444–450.e1.
-
15 ↑
ElbabaaSK,GildehausAM,PiersonMJ,AlbersJA,VlastosEJ.First 60 fetal in-utero myelomeningocele repairs at Saint Louis Fetal Care Institute in the post-MOMS trial era: hydrocephalus treatment outcomes (endoscopic third ventriculostomy versus ventriculo-peritoneal shunt).Childs Nerv Syst.2017;33(7):1157–1168.
-
16 ↑
OuyangL,GrosseSD,ArmourBS,WaitzmanNJ.Health care expenditures of children and adults with spina bifida in a privately insured U.S. population.Birth Defects Res A Clin Mol Teratol.2007;79(7):552–558.
-
17 ↑
Estevez-OrdonezD,DavisMC,HopsonB,ArynchynaA,RocqueBG,FieggenG,et al.Reducing inequities in preventable neural tube defects: the critical and underutilized role of neurosurgical advocacy for folate fortification.Neurosurg Focus.2018;45(4):E20.
-
18 ↑
KesslerBA,CatalinoMP,QuinseyC,GoodnightW,EltonS.Cost of prenatal versus postnatal myelomeningocele closure for both mother and child at 1 year of life.Neurosurg Focus.2019;47(4):E15.

{kind=link}