
Hydrocephalusis a common disorder in both the pediatric and adult neurosurgical fields. The incidence of congenital hydrocephalus in the United States and Canada has been estimated at 68 per 100,000 births.1Hydrocephalus has been classically defined as any increase in CSF within the skull2or as active distension of the ventricular system of the brain resulting from inadequate passage of CSF from its point of production within the cerebral ventricles to its point of absorption into systemic circulation.3Therefore, there appears to be a close relationship between ventricular size and CSF production. Although recent research has raised doubts about the concept of directed bulk-flow movement of CSF, which involves flow from the choroid plexus into the ventricles and across the arachnoid villi back into the blood,4the choroid plexus is widely recognized as the source of CSF production.5In the neuroscience field, the production and directional flow of CSF have been highlighted along with the glymphatic concept.6In clinical situations, rare cases of choroid plexus papilloma or choroid plexus hyperplasia (CPH) have shown hydrocephalus due to an overproduction of CSF, which is treated with shunt procedures or microsurgical removal.7
正常生长曲线与头围are well-established tools used by physicians to assess abnormal growth patterns. Normal growth curves of intracranial volume based on volumetry performed with CT imaging have been reported,8and those of cerebral ventricular volume have been revealed on the basis of volumetry performed with MRI.9Normal thickness of the choroid plexus has been reported in pediatric10and adult populations,11and aging in adult population was associated with increased choroid plexus volume.12Recently, the volume of the choroid plexus has been highlighted in diseases such as psychotic spectrum disorder,13Alzheimer disease,14multiple sclerosis,15stroke,16and pediatric autism.17However, normal pediatric choroid plexus volume and how it increases in the pediatric population remains unclear.
在这项研究中,我们加入了儿科患者minor head trauma who were previously healthy and underwent head CT scans for measurement of intracranial volume, choroid plexus volume, and lateral ventricles volume. We investigated the relationship among these parameters and created growth curves. Additionally, we evaluated the volumes of these parameters in patients with CPH to assess the degree of abnormality and the impact of surgical interventions.
开云体育世界杯赔率
Patients and Study Setting
In this retrospective study, we enrolled patients who underwent CT imaging for head trauma at Osaka Women’s and Children’s Hospital between March 2006 and May 2023. Because a significant dose-response relationship was observed between pediatric CT–related radiation exposure and brain cancer,18our institution follows guidelines to determine whether CT is performed on children with head trauma.19,20Patients were excluded on the basis of the following criteria: 1) suspicion of abuse, 2) need for craniotomy for decompression within a few days after head injury, 3) cranial depressed fracture requiring a recovery operation, 4) obvious compression and apparent deformation of the lateral ventricles due to hematoma, 5) Ommaya reservoir implantation or drainage surgical procedures, 6) presence of complications such as craniosynostosis, tumor, epilepsy, autism, intracranial arachnoid cyst, chromosomal abnormalities, cardiovascular disease, endocrine disorders, etc., and 7) presence of cavum vergae or cavum septum. Therefore, all subjects were healthy prior to head injury, experiencing only minor trauma, and did not require any surgical interventions.
Multiple follow-up CT scans were conducted in some cases due to medical necessity. However, not all scans were included in the analysis because our primary focus was to determine normal growth curves rather than to correlate growth with head trauma. To select the appropriate scans, we established the following criteria: 1) for patients younger than 1 year with multiple scans taken at different ages (in months), one CT scan was evaluated for each month; 2) for patients older than 1 year with multiple scans taken at different ages (in years), one CT scan was evaluated for each year; and 3) for patients with multiple scans obtained at different ages (in months or years), we evaluated only the scan with the least influence from the head injury.
The Ethics Committee of Osaka Women’s and Children’s Hospital, Izumi, Japan, provided ethical approval for this study, which was conducted in accordance with the Declaration of Helsinki guidelines for experiments involving humans. Informed consent was obtained using the opt-out method from our center’s website because of the retrospective and noninvasive nature of the study.
Data Collection
We conducted a retrospective analysis of CT scans and assessed various medical variables, including sex, age, modified Pediatric Glasgow Coma Scale (mPGCS) score,21and CT findings. For quantitative assessment of intracranial volume, choroid plexus volume, and lateral ventricles volume, DICOM CT data were imported to MATLAB R2020b (MathWorks) and the target areas were segmented manually using the Image Segmenter app in MATLAB (https://www.mathworks.com/help/images/ref/imagesegmenter-app.html).Representative segmentation of intracranial volume, choroid plexus volume, and lateral ventricles volume is shown inSupplementary Fig. 1.
The width of each DICOM slice was 5 mm. Choroid plexus observed in the bilateral ventricles and at the foramen of Monro was assessed as a representation of intracranial choroid plexus. The volume of the lateral ventricles was measured as the volume of the bilateral ventricles. These procedures enabled us to calculate the volume (in milliliters) related to the abovementioned parameters, and this method has been used in our other studies.22,23
Statistical Analysis
Categorical data were presented as number (percent). Continuous variables with a normal distribution were presented as mean ± SD, whereas those with a nonnormal distribution were presented as median with 25%–75% quartiles. Spearman correlation coefficients were calculated to evaluate the correlations among parameters.
考虑到年龄分布不均匀,我们屁股essed the distribution and defined age-related clusters for adjustment. Mean and 95% CI of the parameters were calculated, and differences between age-related clusters or sexes were compared by assessing overlapping or nonoverlapping CIs. Nonoverlapping CIs were considered an indicator of statistical significance, whereas overlapping CIs were interpreted as indicative of lack of statistical significance.24Additionally, the unpaired t-test was used to compare age-related clusters, and Bonferroni correction was applied for the correction of multiple comparisons. The statistical difference between clusters was considered significant at corrected p < 0.05.
The measurements of each parameter were plotted according to months after birth, and the best-fitting logarithmic curves were plotted. Statistical analyses were performed using the Statistical and Machine Learning Toolbox of MATLAB R2020b.
Choroid Plexus Hyperplasia
We collected data from patients with CPH who underwent surgical procedures at our institution between March 2006 and May 2023. The volumes of the parameters were calculated and z-normalized by subtracting the mean values and dividing by the SD of the corresponding age-related clusters.
Data Availability
All data in this study are available from the corresponding author upon reasonable request and after additional ethics approval.
Results
Baseline Characteristics
A total of 277 patients were initially enrolled, but 93 patients were subsequently excluded. Among the remaining 184 patients, 1 patient aged 13 years was excluded as an outlier, resulting in the inclusion of 229 CT scans from 183 patients younger than 10 years of age for evaluation (Fig. 1).Of these CT scans, 94 (41.0%) were obtained from female patients, and the median (range) time interval after birth was 12 (6–43) months. Two CT scans were performed in 40 patients (17 females [42.5%]), and 3 CT scans were performed in 3 patients (0 female [0.0%]).

Patient enrollment and CT scans investigated in this study. This flowchart illustrates the inclusion and exclusion criteria for pediatric patients with head trauma who were investigated in this study. Initially, 277 patients were included, but 93 patients were subsequently excluded. Among the remaining patients, only 1 patient was older than 11 years (specifically 13 years old) and was therefore excluded. Consequently, a total of 183 patients were enrolled. On the basis of our criteria for selecting multiple CT scans, a total of 229 CT scans were obtained for analysis.
The majority of the CT scans had an mPGCS value of 15, as observed in 195 scans (85.2%). mPGCS values of 14 were found in 28 scans (12.2%), and values between 9 and 13 were observed in 6 scans (2.6%). Fractures were present in 107 scans (46.7%), including 99 linear fractures (92.5%) and 8 depressed fractures (7.5%). Intracranial bleeding was observed in 67 scans (29.3%), consisting of 33 acute subdural hematomas (49.3%), 26 acute epidural hematomas (38.8%), 13 subarachnoid hemorrhages (19.4%), 3 intracerebral hematomas (4.5%), and 2 intraventricular hemorrhages (3.0%). There were 6 cases of duplicated data points and 2 cases of triplicated data points.
Correlation Analysis
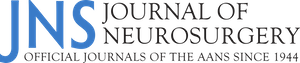
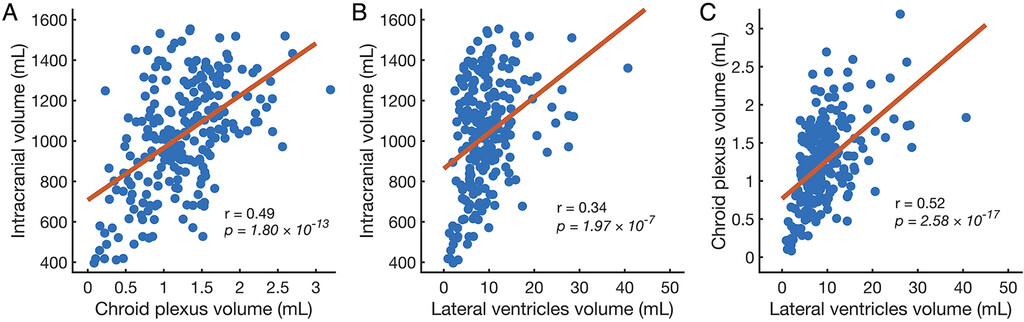
Positive correlations were observed among 3 parameters—intracranial volume, choroid plexus volume, and lateral ventricles volume—in all 3 combinations (Fig. 2).值得注意的是,相关系数ficient between choroid plexus and lateral ventricles volumes reached the highest value, which was significant (r = 0.52, p = 2.58 × 10−17) (Fig. 2C).
Correlations between parameters. Scatter plots between intracranial volume and choroid plexus volume (A), intracranial volume and lateral ventricles volume (B), and choroid plexus volume and lateral ventricles volume (C) are presented. The regression lines are indicated asred lines, andrrepresents the correlation coefficients. Figure is available in color online only.
Age-Related Clusters
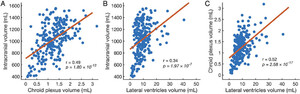
To account for the uneven distribution of the population across different age groups, we categorized the CT scans into 15 age-related clusters: 0 months, 1 month, 2–3 months, 4–5 months, 6–7 months, 8–9 months, 10–11 months, 1 year–1 (i.e., age range 12–17 months), 1 year–2 (i.e., age range 18–23 months), 2 years, 3 years, 4 years, 5–6 years, 7–8 years, and 9–10 years. The number of CT scans performed in each cluster for both males and females is presented inFig. 3. The population distribution between males and females was uneven due to a higher frequency of CT scans for head trauma in males compared with females.
Distribution of the population based on age-related clusters. Fifteen age-related clusters were defined, ranging from 0 months (m) to 9–10 years (y).The cluster labeled as1y-1corresponds to an age range of 12 to 17 months, and the cluster labeled as1y-2corresponds to an age range of 18 to 23 months. Figure is available in color online only.
Sequential Plots of Parameters
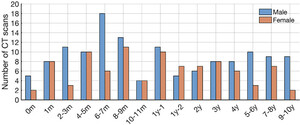
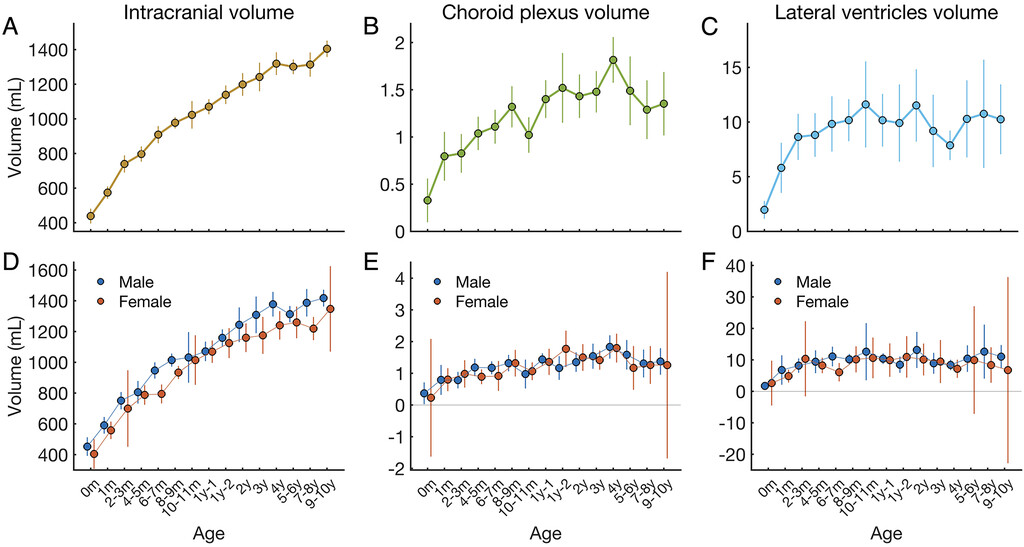
The mean values of each cluster, calculated from the total number of CT scans, were plotted sequentially for intracranial volume (Fig. 4A), choroid plexus volume (Fig. 4B), and lateral ventricles volume (Fig. 4C).Intracranial volume consistently increased step-by-step with each age-related cluster, whereas both choroid plexus and lateral ventricles volume increased until approximately 1 year of age, after which the subsequent rate of increase slowed down. Regarding intracranial volume, the 95% CIs showed almost no overlap among clusters. However, regarding the choroid plexus and lateral ventricles volumes, the 95% CIs after 1 year of age almost showed overlap.
Sequential plots of mean values. The mean values were calculated for each age-related cluster and sequentially plotted for the 3 parameters. Thepanels of the upper rowwere based on all CT scans (A–C), and thepanels of the lower rowwere based on CT scans in males and females (D–F).Error barsindicate 95% CIs. Figure is available in color online only.
The plots generated from males and females are shown in the lower row ofFig. 4. Except for the error bars for intracranial volume at ages 6–7 months, 8–9 months, and 7–8 years (Fig. 4D), the error bars of the males and females showed overlap in each cluster. We noted that the 95% CIs had negative values due to the small number of included females (Fig. 4E–F).Therefore, in this study, we could not determine any differences between males and females due to the small sample sizes; in the following analyses, we present the results obtained from all CT scans.
We plotted the sequential temporal volume changes observed in each patient who underwent multiple CT scans (Supplementary Fig. 2).We observed an increase in intracranial volume over time. However, some patients showed a decrease in choroid plexus and lateral ventricles volumes.
Statistical Differences Among Age-Related Clusters
To compare the volumes between two different age-related clusters for each parameter, we performed the unpaired t-test. To account for multiple comparisons, we applied Bonferroni correction by multiplying the obtained p values by 105, which was the total number of combinations [15C2= (15 × 14)/2]. The significant differences in volume, with corrected p values less than 0.05, were presented as a color-scaled matrix (Fig. 5).We observed significant differences in intracranial volume between two different age-related clusters with patients younger than 2 years of age (Fig. 5A).However, except for the combinations of 0 months and the other age-related clusters, we found almost no significant differences between clusters in terms of choroid plexus and lateral ventricles volumes (Fig. 5B–C).
Color-scaled matrix of significant differences in volume. Differences among the age-related clusters in terms of intracranial volume (A), choroid plexus volume (B), and lateral ventricles volume (C) are presented as a color-scaled matrix. Positive differences, indicating larger volumes in the longitudinal axis compared to the horizontal axis, are colored ingreentoyellow. Negative differences, indicating smaller volumes in the longitudinal axis compared to the horizontal axis, are colored inblue. Only differences that were significant with corrected p values < 0.05 are colored. n.s. = not significant. Figure is available in color online only.
Growth Curve
Scatter plots against age in months were used to generate the best-fitting logarithmic curves: y = 196.99 log (x + 1) + 496.60 for intracranial volume (Fig. 6A), y = 0.20 log (x + 1) + 0.71 for choroid plexus volume (Fig. 6B), and y = 0.90 log (x + 1) + 6.90 for lateral ventricles volume (Fig. 6C).For intracranial volume, the growth rate was faster until approximately 20 months of age and then slowed down after 20 months. However, for choroid plexus and lateral ventricles volume, the growth rate slowed down quickly by approximately 10 months of age.
Scatter plots and growth curves. Scatter plots with age in months along the x-axis are presented for intracranial volume (A), choroid plexus volume (B), and lateral ventricles volume (C).The best-fitting logarithmic curves are indicated asred curves. Figure is available in color online only.
Cases With CPH
Three cases with CPH were included in this study.
Patient 1. Patient 1 (P1) presented to our department at 3 years 4 months of age with abnormal head enlargement. Head CT revealed hydrocephalus and choroid plexus enlargement. She underwent ventriculoperitoneal shunt (VPS) placement and was diagnosed with trisomy 9p. Follow-up for 16 years showed no complications after VPS placement. The size of the enlarged choroid plexus remained unchanged on CT imaging, leading to the diagnosis of CPH.
Patient 2. Patient 2 (P2) was diagnosed with head enlargement at 4 months after birth and was referred to our department. Head CT imaging revealed hydrocephalus and choroid plexus enlargement. At 5 months of age, she underwent VPS placement. At 1 year of age, she developed refractory ascites and underwent external ventricular drainage (EVD). Daily production of CSF was approximately 2400 ml. One week later, ventriculoatrial shunt (VAS) placement was performed. Staged bilateral plexectomy was conducted between 2 and 4 months later, with pathological examination confirming CPH. The VAS was removed after the procedure. She has been monitored for 8 years without any medical problems.
Patient 3. Patient 3 (P3), with trisomy 9p and partial trisomy 9q, had been under the care of our hospital’s department of medical genetics. At 1 year of age, he was referred to our department owing to hydrocephalus. Head CT imaging revealed choroid plexus enlargement, leading to the decision to perform VPS placement combined with bilateral endoscopic plexus coagulation (BEC). Pathological examination confirmed CPH.Supplementary Figure 3displays CT and MRI scans obtained after the operations, showing similar volumes for the choroid plexus and lateral ventricles. Two weeks later, the patient experienced surgical wound dehiscence and developed meningitis. EVD was performed, and meningitis was treated with antibiotics. The daily production of CSF was approximately 2000 ml. After recovering from meningitis, he was transferred to another hospital, where he underwent one-stage bilateral plexectomy.
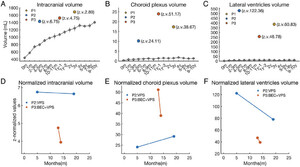
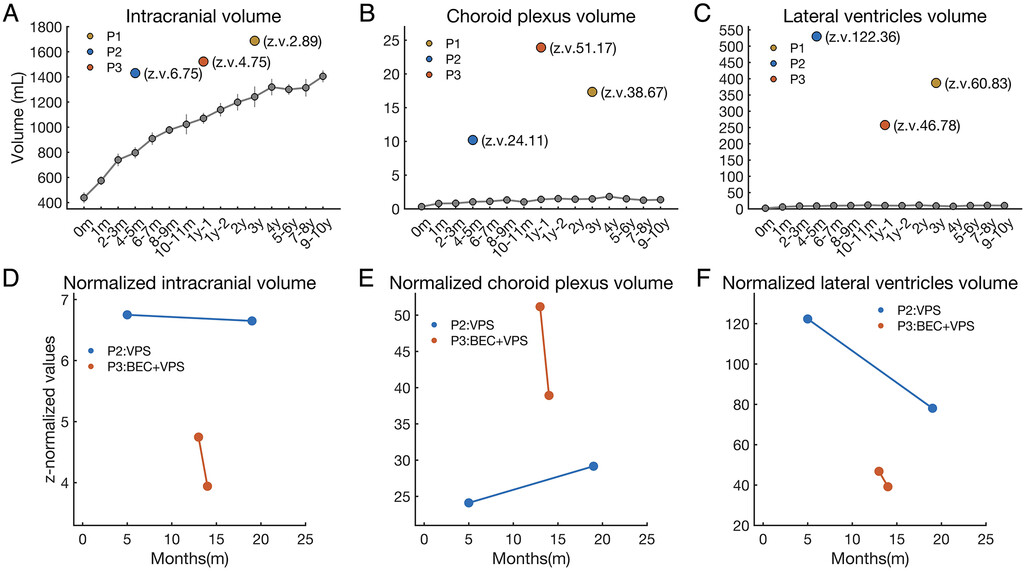
Their profiles are summarized inTable 1. The volumes of the parameters were calculated and z-normalized using the mean and SD values obtained from normal age–related clusters (Supplementary Table 1).The results were plotted over the plots calculated from the normal groups (Fig. 7A–C).The z-normalized values of the choroid plexus and lateral ventricles volumes were notably larger than those of intracranial volume.
Clinical profiles of the patients with CPH
| Patient No. | Sex | Age at Diagnosis of CPH | Preop Intracranial Vol (z.v.) | Preop Choroid Plexus Vol (z.v.) | Preop Lateral Ventricles Vol (z.v.) | 1st Procedure | Complications | Further Procedures | Daily CSF Production (ml) | Definitive Procedure | Genetic Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P1 | F | 3岁4金属氧化物半导体 | 1687.8 ml (2.89) | 17.3 ml (38.67) | 386.9 ml (60.83) | VPS | No | Trisomy 9p | |||
| P2 | F | 5 mos | 1430.5 ml (6.75) | 10.2 ml (24.11) | 530.1 ml (122.36) | VPS | Ascites | EVD, VAS | 2400 | SBP | |
| P3 | M | 1 yr 1 mo | 1522.4 ml (4.75) | 23.9 ml (51.17) | 257.6 ml (46.78) | BEC + VPS | SWD + meningitis | EVD | 2000 | OSBP | Trisomy 9p + partial trisomy 9q |
OSBP = one-stage bilateral plexectomy; SBP = staged bilateral plexectomy; SWD = surgical wound dehiscence; z.v. = z-normalized value.
Results from cases with CPH. Volumes calculated from the patients with CPH for each parameter are presented in theupper row(A–C), with plots and lines calculated from normal age-related clusters indicated ingray, similar to theupper panelsofFig. 3. The changes of the z-normalized values of P2 and P3 for each parameter are presented in thelower row(D–F).z.v. = z-normalized value. Figure is available in color online only.
Specifically, for P2 and P3, the changes in the z-normalized values from the time of initial diagnosis of CPH to the time of EVD are presented in Figs. 7D–F. The z-normalized values of intracranial volume and lateral ventricles volume decreased. In the case of P3, the z-normalized choroid plexus volume decreased from 51.17 to 38.93 (23.9% decrease) due to BEC.
Discussion
Using CT scans from Japanese pediatric patients with minor head trauma, we generated normal growth curves for intracranial volume, choroid plexus volume, and lateral ventricles volume. Positive correlations were observed among these parameters. The growth rate of intracranial volume was rapid until approximately 20 months of age, while the growth rates of choroid plexus and lateral ventricles volumes slowed down by approximately 1 year of age. Subsequently, the volumes of choroid plexus and lateral ventricles stabilized at around 1.5 ml and 10 ml, respectively. We utilized z-normalization to objectively assess hydrocephalus caused by CPH and its impact of surgical procedures.
Although MRI is commonly used to assess the volume of the ventricles9or choroid plexus,13–17,25–27we chose to utilize CT imaging in our evaluation. The border between the choroid plexus and ventricle wall is more clearly defined with MRI, while it appears less distinct with CT imaging (Supplementary Figs. 1and3).Consequently, MRI is considered the superior method for choroid plexus assessment. However, obtaining head MRI from healthy children without underlying conditions can be challenging. Hence, we utilized CT scans from pediatric patients with minor head trauma and no pre-existing health issues. The volumes calculated from the CT scans of P3 showed similar values to those obtained from MRI (Supplementary Fig. 3).A previous MRI study reported a mean choroid plexus volume of approximately 1.2 ml in adult control groups,16which aligns with our findings. Moreover, because only one evaluator (H.H.) segmented the choroid plexus, there was consistency in our measurements. Additionally, a previous MRI study indicated that the 50th percentile of ventricular volume after 1 year of age was approximately 10 ml, with rapid growth occurring in the 1st year of life.9This is consistent with our results. Although we used CT scans with a 5-mm slice width and had concerns about lower resolution, a previous CT study that employed a slice width of 2 mm or less reported normal pediatric growth curves for intracranial volume,8similar to our findings. These consistencies between previous findings and our results validate our methodology and outcomes. However, it is important to note that the use of CT is a limitation of this study.
Posttraumatic hydrocephalus, with an incidence ranging from 0.7% to 50%, can develop after a brain injury.28,29InSupplementary Fig. 2, we show a temporal reduction in choroid plexus and lateral ventricles volumes. This led us to suspect that the initially enlarged ventricles after head injury might return to a normal state. Previous studies have reported a positive correlation between choroid plexus and lateral ventricles volumes,13,17,27我们还发现。然而,因果关系between these volumes remains unclear. Although it is natural for a large volume of choroid plexus to induce a large volume of the lateral ventricles in patients with CPH, larger ventricles could potentially overestimate choroid plexus volume. Because the choroid plexus is a soft tissue, its size is likely to vary depending on the size of the ventricles. Consequently, cases with larger lateral ventricles, possibly due to head trauma, exhibited larger choroid plexus volumes. In this study, we assumed that minor head trauma had no impact on the growth of the intracranial structures. Further research is needed to explore this relationship. It is important to acknowledge that the inclusion of patients with head trauma is a significant limitation of this study.
We categorized the pediatric patients into age-related clusters and calculated volumes within each cluster. Mean and SD values were obtained for each cluster (Supplementary Table 1), and these were used to calculate z-normalized values. A z-normalization approach is commonly used to compare groups with different baseline values, such as with electroencephalogram-related frequency analysis.30In the field of pediatric neurosurgery, because the baseline values of intracranial volume vary among patients of different ages, we found that z-normalization was useful for comparing volumes across different age groups. Adult studies have assessed variability in head size. For example, choroid plexus volume was corrected for intracranial volume,12and the 2-dimensional Evans index has been used to evaluate normal pressure hydrocephalus. However, the limitations of the Evans index have been noted,31,32and the importance of 3-dimensional assessment has been emphasized.9Our study provides normal volume values, which are 3-dimensional data and have the potential to enable assessment of pediatric hydrocephalus while accounting for the growth of intracranial structures. Specifically, because we demonstrated the rapid rate of growth of the choroid plexus and lateral ventricles until 1 year of age, we believe that accounting for normal growth is essential to the assessment of pediatric hydrocephalus in patients younger than 1 year.
Although there are no established radiological criteria for defining the dimensions of a normal choroidal plexus or CPH,7,33从而导致主观的诊断,我们艾梅d to provide an objective assessment of CPH. In the case of P1, although the actual intracranial volume was the highest among the 3 patients, its z-normalized value was the lowest. In the case of P2, the z-normalized choroid plexus volume increased due to growth after VPS treatment, while the z-normalized intracranial volume and lateral ventricles volume improved. In the case of P3, BEC was added to VPS treatment, resulting in a reduction of approximately 24% in z-normalized choroid plexus volume and improvement in z-normalized intracranial volume and lateral ventricles volume. These changes likely reflected the effect of VPS or BEC. Our findings have the potential to provide an objective assessment of abnormal volumes in hydrocephalus or choroid plexus disorders, such as CPH, choroid plexus papilloma, and choroid plexus carcinoma. However, further studies are needed to demonstrate the usefulness of our normal growth curves for objective assessment of the effects of surgery.
Our findings indicate that the choroid plexus exhibits rapid growth until 1 year of age, reaching a volume of approximately 1.5 ml. After this point, it reaches a plateau. Interestingly, a previous study reported a different trend, with choroid plexus volume decreasing between the ages of 5 and 10 years and then stabilizing.17Furthermore, the calculated mean choroid plexus volume in the adult control groups was approximately 1.2 ml,16and it has been noted that choroid plexus volume increases with age after 50 years.12These findings suggest that the growth rate of choroid plexus volume is rapid until approximately 1 year of age, averaging 1.5 ml, followed by a decrease to an average of 1.2 ml and subsequent stabilization. Additionally, there may be a resurgence in the growth of choroid plexus volume after the age of 50 years.
CPH is a rare pediatric disorder characterized by the overproduction of CSF. Trisomy 9p and tetrasomy 9p have been associated with CPH, as genes on chromosome 9p are likely involved in the regulation of choroid plexus growth.33In our study, 2 of 3 patients in our study showed trisomy 9p. Although VPS placement is the initial treatment for most cases, nearly all CPH patients experience complications such as refractory ascites, often necessitating additional procedures such as BEC or choroid plexus removal.7CSF production exceeding 2000 ml daily has been reported,7,34–36and it has been suggested that hydrocephalus caused by villous hyperplasia of the choroid plexus can be resolved with a VAS if CSF production does not exceed 1000 ml/day.37In our study, 1 patient was successfully treated with VPS placement alone, while the other 2 patients with daily CSF production exceeding 2000 ml experienced complications. One of these patients developed meningitis, which is known to decrease CSF absorption due to an inflammatory response.29This may have worsened the patient’s hydrocephalus and increased the daily drained CSF volume. Considering the challenges that we encountered with VPS-related complications in CPH patients, it is crucial for neurosurgeons to identify factors that render VPS ineffective for CHP-related hydrocephalus.
Although our study did not reveal significant differences between males and females, it is important to acknowledge that our sample size, especially for females, may have been insufficient to detect sex-related differences. The proportion of females in our study was approximately 40%, which could be lower than the proportion of males due to the enrollment of children with head trauma. A previous study that investigated head injury in individuals aged 15 to 79 years reported that females consisted of only 23% of the study population.38These findings suggest that males have a higher incidence rate of head trauma compared with females in both pediatric and adult populations. However, previous studies that evaluated adult or pediatric ventricular volume reported no significant effect of sex12or slightly lower ventricular volumes in females compared with males.9Therefore, it is possible that there may be no statistical differences in the growth of intracranial volume, choroid plexus volume, and lateral ventricles volume between sexes.
我们的研究有一些额外的限制。首先,we were unable to collect data on low-birth-weight infants, which could have influenced the growth curves presented in our study. Secondly, our study included data from only Japanese children, so there is a possibility that racial differences may have impacted our results. However, because our findings were consistent with those from other populations,9,16we believe that these differences can be disregarded. Lastly, our study provided only results for children as old as 10 years of age, and the growth curves for children older than 10 years are still unknown.
Conclusions
Our study, conducted on Japanese pediatric patients with minor head trauma, provides normal growth curves for intracranial volume, choroid plexus volume, and lateral ventricles volume. Choroid plexus volume and lateral ventricles volume demonstrated rapid increases until 1 year of age, reaching approximately 1.5 ml and 10 ml, respectively, and plateauing thereafter. Using z-normalization, we demonstrated the potential for objective assessment of hydrocephalus severity in CPH patients and the evaluation of surgical intervention effectiveness. Our findings contribute to the objective evaluation of hydrocephalus and choroid plexus–related disorders while considering the growth patterns of children. Objective assessments have the potential to unveil factors associated with complications after CPH surgical procedures, providing crucial insights for neurosurgeons planning interventions for CPH patients.
Acknowledgments
The Japan Society for the Promotion of Science (KAKENHI JP21K16629 awarded to H.H.) supported this work.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Author Contributions
概念和设计:桥本,千叶。Acquisition of data: all authors. Analysis and interpretation of data: Hashimoto. Drafting the article: Hashimoto. Critically revising the article: Hashimoto, Chiba. Reviewed submitted version of manuscript: Hashimoto, Chiba. Approved the final version of the manuscript on behalf of all authors: Hashimoto. Statistical analysis: Hashimoto. Administrative/technical/material support: Hashimoto, Takemoto, Chiba. Study supervision: Takemoto, Chiba.
Supplemental Information
Online-Only Content
Supplemental material is available with the online version of the article.
Supplementary Figures and Table.//www.prize-show.com/doi/suppl/10.3171/2023.7.PEDS23218.
Data Availability
All data in this study are available from the corresponding author upon reasonable request and after additional ethics approval.
Preprint Server
An earlier version of this article can be found on a preprint server.
Preprint server name: medRxiv.
Preprint DOI: 10.1101/2023.05.10.23289689v1.
References
-
1 ↑
DewanMC,RattaniA,MekaryR,et al.Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis.J Neurosurg.2018;130(4):1065–1079.
-
2 ↑
RaimondiAJ.A unifying theory for the definition and classification of hydrocephalus.Childs Nerv Syst.1994;10(1):2–12.
-
3 ↑
RekateHL.The definition and classification of hydrocephalus: a personal recommendation to stimulate debate.Cerebrospinal Fluid Res.2008;5(1):2.
-
4 ↑
BrinkerT,StopaE,MorrisonJ,KlingeP.A new look at cerebrospinal fluid circulation.Fluids Barriers CNS.2014;11(1):10.
-
5 ↑
MacAulayN,KeepRF,ZeuthenT.Cerebrospinal fluid production by the choroid plexus: a century of barrier research revisited.Fluids Barriers CNS.2022;19(1):26.
-
6 ↑
MestreH,MoriY,NedergaardM.The brain’s glymphatic system: current controversies.Trends Neurosci.2020;43(7):458–466.
-
7 ↑
HallaertGG,VanhauwaertDJ,LoggheK,et al.Endoscopic coagulation of choroid plexus hyperplasia.J Neurosurg Pediatr.2012;9(2):169–177.
-
8 ↑
TomitaY,KamedaM,SenooT,et al.Growth curves for intracranial volume and two-dimensional parameters for Japanese children without cranial abnormality: toward treatment of craniosynostosis.神经医学Chir (Tokyo).2022;62(2):89–96.
-
9 ↑
CutlerNS,SrinivasanS,AaronBL,et al.Normal cerebral ventricular volume growth in childhood.J Neurosurg Pediatr.2020;26(5):517–524.
-
10 ↑
MadhukarM,ChoudharyAK,BoalDK,DiasMS,IantoscaMR.Choroid plexus: normal size criteria on neuroimaging.Surg Radiol Anat.2012;34(10):887–895.
-
11 ↑
İmamoğluH,ErkoçM,Şalkİ,et al.Evaluation of the normal choroid plexus size in adults with magnetic resonance imaging.Cumhur Medical J.2013;35(1):51–54.
-
12 ↑
AlischJSR,KielyM,TriebswetterC,et al.Characterization of age-related differences in the human choroid plexus volume, microstructural integrity, and blood perfusion using multiparameter magnetic resonance imaging.Front Aging Neurosci.2021;13:734992.
-
13 ↑
LizanoP,LutzO,LingG,et al.Association of choroid plexus enlargement with cognitive, inflammatory, and structural phenotypes across the psychosis spectrum.Am J Psychiatry.2019;176(7):564–572.
-
14 ↑
ChoiJD,MoonY,KimHJ,YimY,LeeS,MoonWJ.Choroid plexus volume and permeability at brain MRI within the Alzheimer disease clinical spectrum.Radiology.2022;304(3):635–645.
-
15 ↑
MüllerJ,SinneckerT,WendebourgMJ,et al.Choroid plexus volume in multiple sclerosis vs neuromyelitis optica spectrum disorder: a retrospective, cross-sectional analysis.Neurol Neuroimmunol Neuroinflamm.2022;9(3):e1147.
-
16 ↑
EgorovaN,GottliebE,KhlifMS,SprattNJ,BrodtmannA.Choroid plexus volume after stroke.Int J Stroke.2019;14(9):923–930.
-
17 ↑
LevmanJ,VasungL,MacDonaldP,et al.Regional volumetric abnormalities in pediatric autism revealed by structural magnetic resonance imaging.Int J Dev Neurosci.2018;71:34–45.
-
18 ↑
HauptmannM,ByrnesG,CardisE,et al.脑癌从CT辐射暴露后考试inations of children and young adults: results from the EPI-CT cohort study.Lancet Oncol.2023;24(1):45–53.
-
19 ↑
MuhmM,DankoT,HenzlerT,LuizT,WinklerH,RuffingT.Pediatric trauma care with computed tomography—criteria for CT scanning.Emerg Radiol.2015;22(6):613–621.
-
20 ↑
AstrandR,RosenlundC,UndénJ.Scandinavian guidelines for initial management of minor and moderate head trauma in children.BMC Med.2016;14(1):33.
-
22 ↑
HashimotoH,MaruoT,KimotoY,et al.The association between diffusion-weighted imaging—Alberta Stroke Program Early Computed Tomography Score and the outcome following mechanical thrombectomy of anterior circulation occlusion.Interdiscip Neurosurg.2023;33:101758.
-
23 ↑
HashimotoH,MaruoT,KimotoY,NakamuraM,FujinagaT,UshioY.Burr hole locations are associated with recurrence in single burr hole drainage surgery for chronic subdural hematoma.World Neurosurg X.2023;19:100204.
-
24 ↑
GaoK,KempDE,GanocySJ,GajwaniP,XiaG,CalabreseJR.Antipsychotic-induced extrapyramidal side effects in bipolar disorder and schizophrenia: a systematic review.J Clin Psychopharmacol.2008;28(2):203–209.
-
25 ↑
AlischJSR,EganJM,BouhraraM.Differences in the choroid plexus volume and microstructure are associated with body adiposity.Front Endocrinol (Lausanne).2022;13:984929.
-
26
RiciglianoVAG,MorenaE,ColombiA,et al.Choroid plexus enlargement in inflammatory multiple sclerosis: 3.0-T MRI and translocator protein PET evaluation.Radiology.2021;301(1):166–177.
-
27 ↑
TadayonE,Pascual-LeoneA,PressD,SantarnecchiE.Choroid plexus volume is associated with levels of CSF proteins: relevance for Alzheimer’s and Parkinson’s disease.Neurobiol Aging.2020;89:108–117.
-
28 ↑
De BonisP,AnileC.Post-traumatic hydrocephalus: the Cinderella of Neurotrauma.Expert Rev Neurother.2020;20(7):643–646.
-
29 ↑
KhasawnehAH,GarlingRJ,HarrisCA.Cerebrospinal fluid circulation: What do we know and how do we know it?Brain Circ.2018;4(1):14–18.
-
30 ↑
HashimotoH,KhooHM,YanagisawaT,et al.Frequency band coupling with high-frequency activities in tonic-clonic seizures shifts from θ to δ band.Clin Neurophysiol.2022;137:122–131.
-
31 ↑
BrixMK,WestmanE,SimmonsA,et al.The Evans’ Index revisited: new cut-off levels for use in radiological assessment of ventricular enlargement in the elderly.Eur J Radiol.2017;95:28–32.
-
32 ↑
TomaAK,HollE,KitchenND,WatkinsLD.Evans’ index revisited: the need for an alternative in normal pressure hydrocephalus.开云体育app官方网站下载入口.2011;68(4):939–944.
-
33 ↑
FureyC,AntwiP,DuranD,et al.9p24 triplication in syndromic hydrocephalus with diffuse villous hyperplasia of the choroid plexus.Cold Spring Harb Mol Case Stud.2018;4(5):a003145.
-
34 ↑
CaseyKF,VriesJK.Cerebral fluid overproduction in the absence of tumor or villous hypertrophy of the choroid plexus.Childs Nerv Syst.1989;5(5):332–334.
-
35
TamburriniG,CaldarelliM,Di RoccoF,et al.The role of endoscopic choroid plexus coagulation in the surgical management of bilateral choroid plexuses hyperplasia.Childs Nerv Syst.2006;22(6):605–608.
-
36 ↑
FujimuraM,OnumaT,KameyamaM,et al.Hydrocephalus due to cerebrospinal fluid overproduction by bilateral choroid plexus papillomas.Childs Nerv Syst.2004;20(7):485–488.
-
37 ↑
BritzGW,KimDK,LoeserJD.Hydrocephalus secondary to diffuse villous hyperplasia of the choroid plexus. Case report and review of the literature.J Neurosurg.1996;85(4):689–691.
-
38 ↑
FarinA,DeutschR,BiegonA,MarshallLF.Sex-related differences in patients with severe head injury: greater susceptibility to brain swelling in female patients 50 years of age and younger.J Neurosurg.2003;98(1):32–36.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}